

Long term sequelae from childhood pneumonia; systematic review and meta-analysis
- PMID: 22384005
- PMCID: PMC3285155
- DOI: 10.1371/journal.pone.0031239
Long term sequelae from childhood pneumonia; systematic review and meta-analysis
Abstract
Background: The risks of long term sequelae from childhood pneumonia have not been systematically assessed. The aims of this study were to: (i) estimate the risks of respiratory sequelae after pneumonia in children under five years; (ii) estimate the distribution of the different types of respiratory sequelae; and (iii) compare sequelae risk by hospitalisation status and pathogen.
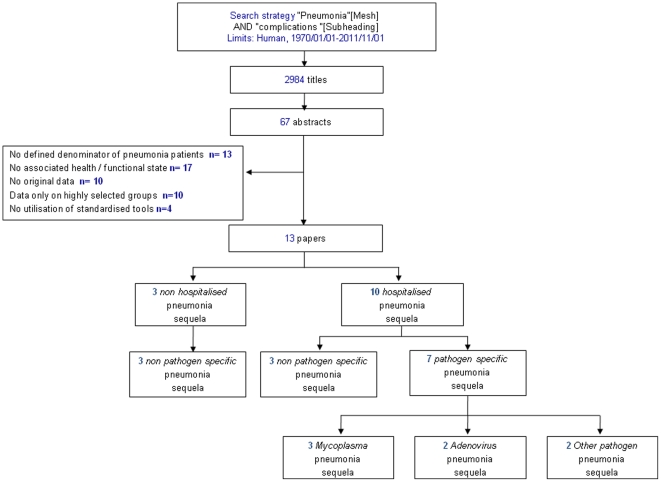
Methods: We systematically reviewed published papers from 1970 to 2011. Standard global burden of disease categories (restrictive lung disease, obstructive lung disease, bronchiectasis) were labelled as major sequelae. 'Minor' sequelae (chronic bronchitis, asthma, other abnormal pulmonary function, other respiratory disease), and multiple impairments were also included. Thirteen papers were selected for inclusion. Synthesis was by random effects meta-analysis and meta-regression.
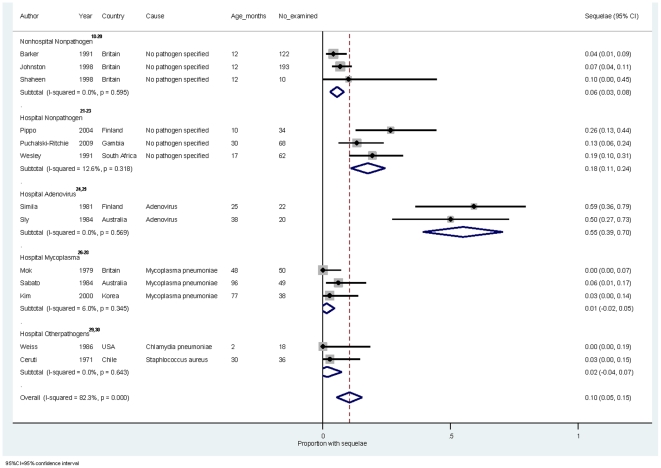
Results: Risk of at least one major sequelae was 5.5% (95% confidence interval [95% CI] 2.8-8.3%) in non hospitalised children and 13.6% [6.2-21.1%]) in hospitalised children. Adenovirus pneumonia was associated with the highest sequelae risk (54.8% [39.2-70.5%]) but children hospitalised with no pathogen isolated also had high risk (17.6% [10.9-24.3%]). The most common type of major sequela was restrictive lung disease (5.4% [2.5-10.2%]) . Potential confounders such as loss to follow up and median age at infection were not associated with sequelae risk in the final models.
Conclusions: All children with pneumonia diagnosed by a health professional should be considered at risk of long term sequelae. Evaluation of childhood pneumonia interventions should include potential impact on long term respiratory sequelae.
Conflict of interest statement
Figures
Similar articles
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2017 Dec 22;12(12):CD011535. doi: 10.1002/14651858.CD011535.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Jan 9;1:CD011535. doi: 10.1002/14651858.CD011535.pub3. PMID: 29271481 Free PMC article. Updated.
-
Antibiotics for exacerbations of asthma.Cochrane Database Syst Rev. 2018 Jun 25;6(6):CD002741. doi: 10.1002/14651858.CD002741.pub2. Cochrane Database Syst Rev. 2018. PMID: 29938789 Free PMC article.
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
Individual-level interventions to reduce personal exposure to outdoor air pollution and their effects on people with long-term respiratory conditions.Cochrane Database Syst Rev. 2021 Aug 9;8(8):CD013441. doi: 10.1002/14651858.CD013441.pub2. Cochrane Database Syst Rev. 2021. PMID: 34368949 Free PMC article.
Cited by
-
Influence of the timing of bronchoscopic alveolar lavage on children with adenovirus pneumonia: a comparative study.BMC Pulm Med. 2021 Nov 11;21(1):363. doi: 10.1186/s12890-021-01708-y. BMC Pulm Med. 2021. PMID: 34763680 Free PMC article.
-
Association of early viral lower respiratory infections and subsequent development of atopy, a systematic review and meta-analysis of cohort studies.PLoS One. 2020 Apr 24;15(4):e0231816. doi: 10.1371/journal.pone.0231816. eCollection 2020. PLoS One. 2020. PMID: 32330171 Free PMC article.
-
Does Measles Vaccination Reduce the Risk of Acute Respiratory Infection (ARI) and Diarrhea in Children: A Multi-Country Study?PLoS One. 2017 Jan 11;12(1):e0169713. doi: 10.1371/journal.pone.0169713. eCollection 2017. PLoS One. 2017. PMID: 28076428 Free PMC article.
-
Air pollution and respiratory infections during early childhood: an analysis of 10 European birth cohorts within the ESCAPE Project.Environ Health Perspect. 2014 Jan;122(1):107-13. doi: 10.1289/ehp.1306755. Epub 2013 Oct 22. Environ Health Perspect. 2014. PMID: 24149084 Free PMC article.
-
Growth and Neurodevelopment of HIV-Exposed Uninfected Children: a Conceptual Framework.Curr HIV/AIDS Rep. 2019 Dec;16(6):501-513. doi: 10.1007/s11904-019-00459-0. Curr HIV/AIDS Rep. 2019. PMID: 31732866 Free PMC article. Review.
References
-
- Glezen P, Denny FW. Epidemiology of acute lower respiratory disease in children. N Engl J Med. 1973;288:498–505. - PubMed
-
- Chang AB, Bell SC, Byrnes CA, Grimwood K, Holmes PW, et al. Chronic suppurative lung disease and bronchiectasis in children and adults in Australia and New Zealand. Med J Aust. 2010;193:356–365. - PubMed
-
- Chang AB, Masel JP, Boyce NC, Wheaton G, Torzillo PJ. Non-CF bronchiectasis: clinical and HRCT evaluation. Pediatr Pulmonol. 2003;35:477–483. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
