

Evidence for altered basal ganglia-brainstem connections in cervical dystonia
- PMID: 22384048
- PMCID: PMC3285161
- DOI: 10.1371/journal.pone.0031654
Evidence for altered basal ganglia-brainstem connections in cervical dystonia
Abstract
Background: There has been increasing interest in the interaction of the basal ganglia with the cerebellum and the brainstem in motor control and movement disorders. In addition, it has been suggested that these subcortical connections with the basal ganglia may help to coordinate a network of regions involved in mediating posture and stabilization. While studies in animal models support a role for this circuitry in the pathophysiology of the movement disorder dystonia, thus far, there is only indirect evidence for this in humans with dystonia.
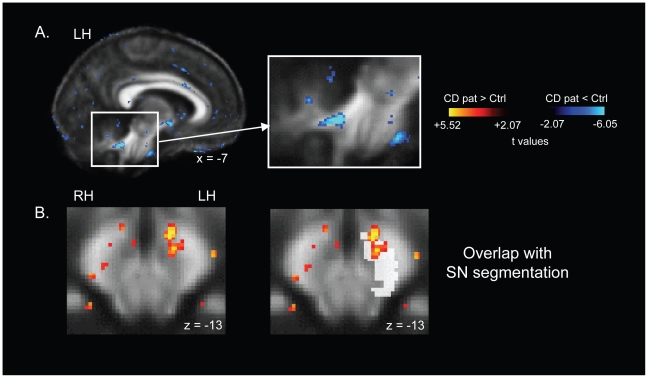
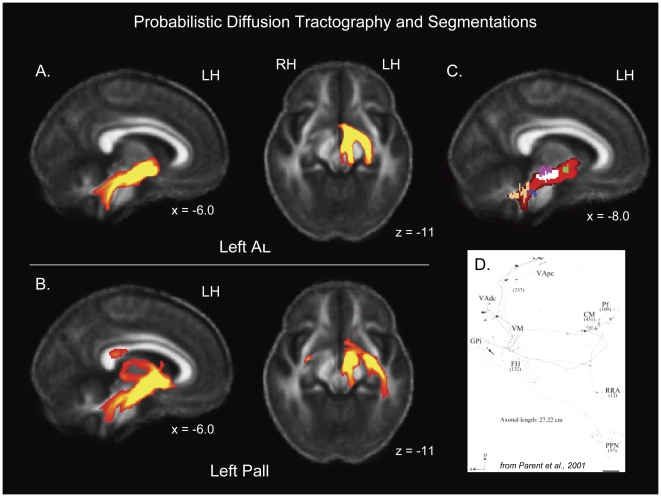
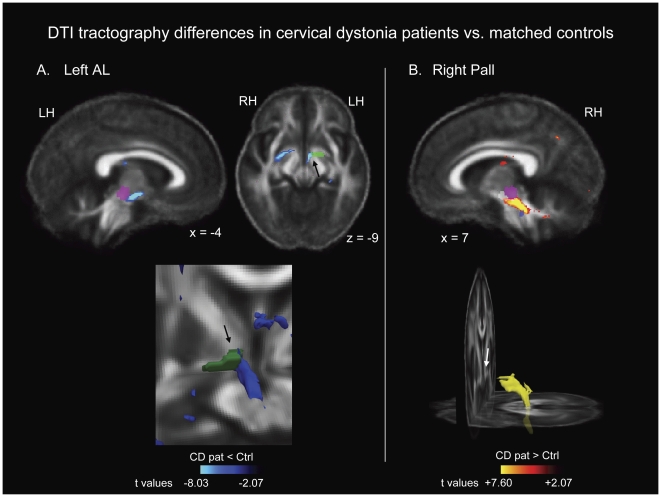
Methodology/principal findings: In the current study we investigated probabilistic diffusion tractography in DYT1-negative patients with cervical dystonia and matched healthy control subjects, with the goal of showing that patients exhibit altered microstructure in the connectivity between the pallidum and brainstem. The brainstem regions investigated included nuclei that are known to exhibit strong connections with the cerebellum. We observed large clusters of tractography differences in patients relative to healthy controls, between the pallidum and the brainstem. Tractography was decreased in the left hemisphere and increased in the right hemisphere in patients, suggesting a potential basis for the left/right white matter asymmetry we previously observed in focal dystonia patients.
Conclusions/significance: These findings support the hypothesis that connections between the basal ganglia and brainstem play a role in the pathophysiology of dystonia.
Conflict of interest statement
Figures
References
-
- Loher TJ, Krauss JK. Dystonia associated with pontomesencephalic lesions. Mov Disord. 2009;24:157–167. - PubMed
-
- Tan EK, Chan LL, Auchus AP. Hemidystonia precipitated by acute pontine infarct. J Neurol Sci. 2005;234:109–111. - PubMed
-
- McNaught KS, Kapustin A, Jackson T, Jengelley TA, Jnobaptiste R, et al. Brainstem pathology in DYT1 primary torsion dystonia. Ann Neurol. 2004;56:540–547. - PubMed
-
- Wu CL, Lu CS. Delayed-onset dystonia following recovery from central pontine myelinolysis. J Formos Med Assoc. 1992;91:1013–1016. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
