

Effect of artificial shrinkage on clinical outcome in fresh blastocyst transfer cycles
- PMID: 22384424
- PMCID: PMC3283060
- DOI: 10.5653/cerm.2011.38.2.87
Effect of artificial shrinkage on clinical outcome in fresh blastocyst transfer cycles
Abstract
Objective: This study aimed to determine the safety and clinical effect of artificial shrinkage (AS) in terms of assisted hatching of fresh blastocysts. Also, we evaluated the correlation between patient age and the effect of AS on clinical outcome.
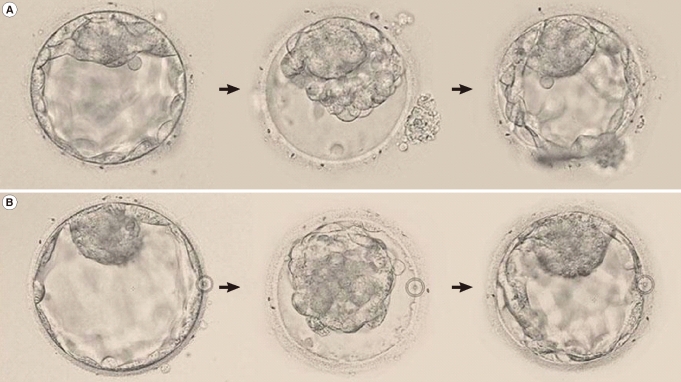
Methods: Two AS methods, using a 29-gauge needle and laser pulse, were compared. Seventy-three blastocysts were shrunk using a 29-gauge needle and the same number of other blastocysts were shrunk by a laser pulse. We evaluated the shrunken blastocysts hourly and considered them viable if they re-expanded >70%. Blastocyst transfer cycles (n=134) were divided into two groups: a control group consisted of the cycles whose intact embryos were transferred (n=100), while the AS group consisted of the cycles whose embryos were replaced following AS (n=34). The implantation and pregnancy rates of the control group and AS group were compared (p<0.05).
Results: The re-expansion rates of the 29-gauge needle and laser pulse AS groups were similar (56 [76.7%] vs. 62 [84.9%], respectively). All of the remaining shrunken blastocysts were re-expanded within 2 hours. There was no degeneration of shrunken blastocysts. The total and clinical pregnancy rate of the AS group (23 [67.6%]; 20 [58.8%], respectively) was significantly higher than that of the control group (47 [47.0%]; 39 [39.0%], respectively). In the older patient group, there was no difference in the clinical outcomes between the AS and control groups.
Conclusion: These results suggest that AS of blastocoele cavity, followed by the transfer, would be a useful approach to improve the clinical outcome in cycles in which fresh blastocyst stage embryos are transferred.
Keywords: Artificial Shrinkage; Assisted Hatching; Embryo Transfer; Human; In Vitro Fertilization.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Houghton FD, Humpherson PG, Hawkhead JA, Hall CJ, Leese HJ. Na+, K+, ATPase activity in the human and bovine preimplantation embryo. Dev Biol. 2003;263:360–366. - PubMed
-
- Biggers JD. Reflections on the culture of the preimplantation embryo. Int J Dev Biol. 1998;42:879–884. - PubMed
-
- Watson AJ, Barcroft LC. Regulation of blastocyst formation. Front Biosci. 2001;6:D708–D730. - PubMed
-
- Veeck LL, Zaninovic N. An atlas of human blastocysts. New York: Parthenon Pub. Group; 2003.
-
- Glass RH, Lin TP, Florence J. Mouse blastocyst re-expansion following puncture and treatment with inhibitors. J Reprod Fertil. 1973;35:533–536. - PubMed
LinkOut - more resources
Full Text Sources
Medical
