

Negative- versus positive-pressure ventilation in intubated patients with acute respiratory distress syndrome
- PMID: 22386062
- PMCID: PMC3681349
- DOI: 10.1186/cc11216
Negative- versus positive-pressure ventilation in intubated patients with acute respiratory distress syndrome
Abstract
Introduction: Recent experimental data suggest that continuous external negative-pressure ventilation (CENPV) results in better oxygenation and less lung injury than continuous positive-pressure ventilation (CPPV). The effects of CENPV on patients with acute respiratory distress syndrome (ARDS) remain unknown.
Methods: We compared 2 h CENPV in a tankrespirator ("iron lung") with 2 h CPPV. The six intubated patients developed ARDS after pulmonary thrombectomy (n = 1), aspiration (n = 3), sepsis (n = 1) or both (n = 1). We used a tidal volume of 6 ml/kg predicted body weight and matched lung volumes at end expiration. Haemodynamics were assessed using the pulse contour cardiac output (PiCCO) system, and pressure measurements were referenced to atmospheric pressure.
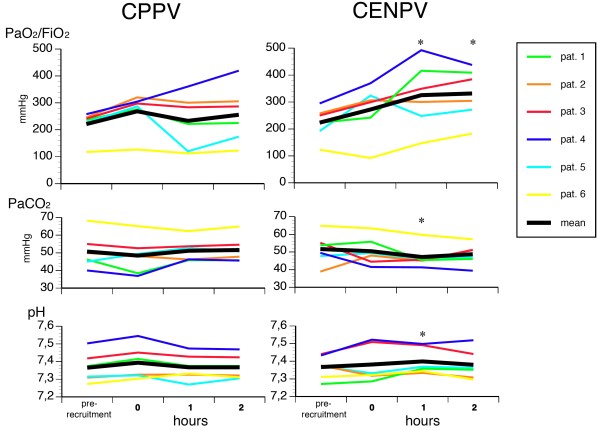
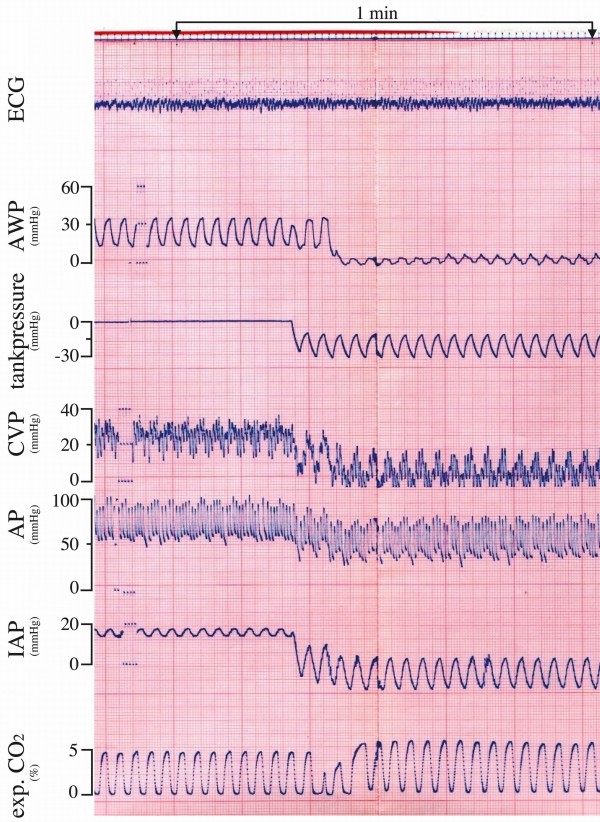
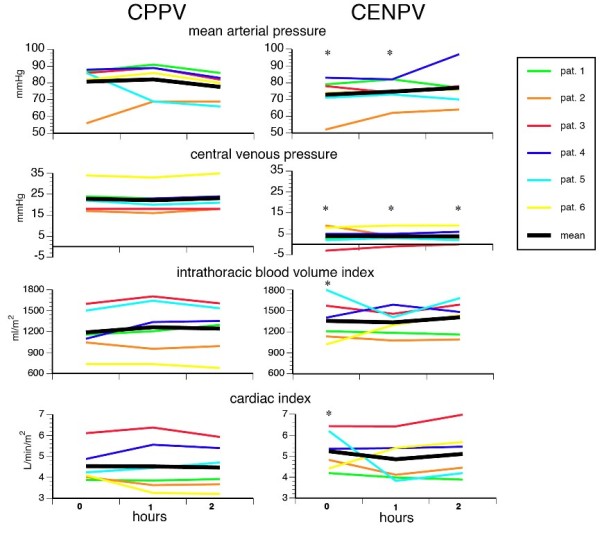
Results: CENPV resulted in better oxygenation compared to CPPV (median ratio of arterial oxygen pressure to fraction of inspired oxygen of 345 mmHg (minimum-maximum 183 to 438 mmHg) vs 256 mmHg (minimum-maximum 123 to 419 mmHg) (P < 0.05). Tank pressures were -32.5 cmH2O (minimum-maximum -30 to -43) at end inspiration and -15 cmH2O (minimum-maximum -15 to -19 cmH2O) at end expiration. NO Inspiratory transpulmonary pressures decreased (P = 0.04) and airway pressures were considerably lower at inspiration (-1.5 cmH2O (minimum-maximum -3 to 0 cmH2O) vs 34.5 cmH2O (minimum-maximum 30 to 47 cmH2O), P = 0.03) and expiration (4.5 cmH2O (minimum-maximum 2 to 5) vs 16 cmH2O (minimum-maximum 16 to 23), P =0.03). During CENPV, intraabdominal pressures decreased from 20.5 mmHg (12 to 30 mmHg) to 1 mmHg (minimum-maximum -7 to 5 mmHg) (P = 0.03). Arterial pressures decreased by approximately 10 mmHg and central venous pressures by 18 mmHg. Intrathoracic blood volume indices and cardiac indices increased at the initiation of CENPV by 15% and 20% (P < 0.05), respectively. Heart rate and extravascular lung water indices remained unchanged.
Conclusions: CENPV with a tank respirator improved gas exchange in patients with ARDS at lower transpulmonary, airway and intraabdominal pressures and, at least initially improving haemodynamics. Our observations encourage the consideration of further studies on the physiological effects and the clinical effectiveness of CENPV in patients with ARDS.
Figures

Similar articles
-
Respiratory and haemodynamic changes during decremental open lung positive end-expiratory pressure titration in patients with acute respiratory distress syndrome.Crit Care. 2009;13(2):R59. doi: 10.1186/cc7786. Epub 2009 Apr 17. Crit Care. 2009. PMID: 19374751 Free PMC article. Clinical Trial.
-
Volume-controlled ventilation and pressure-controlled inverse ratio ventilation: a comparison of their effects in ARDS patients.Monaldi Arch Chest Dis. 1994 Jun;49(3):201-7. Monaldi Arch Chest Dis. 1994. PMID: 8087114 Clinical Trial.
-
[Effect of different transpulmonary pressures guided mechanical ventilation on respiratory and hemodynamics of patients with ARDS: a prospective randomized controlled trial].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2017 Jan;29(1):39-44. doi: 10.3760/cma.j.issn.2095-4352.2017.01.009. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2017. PMID: 28459402 Clinical Trial. Chinese.
-
Experts' opinion on management of hemodynamics in ARDS patients: focus on the effects of mechanical ventilation.Intensive Care Med. 2016 May;42(5):739-749. doi: 10.1007/s00134-016-4326-3. Epub 2016 Apr 1. Intensive Care Med. 2016. PMID: 27038480 Review.
-
[Mechanical ventilation in acute respiratory distress syndrome (ARDS): lung protecting strategies for improved alveolar recruitment].Ned Tijdschr Geneeskd. 2003 Feb 22;147(8):327-31. Ned Tijdschr Geneeskd. 2003. PMID: 12661116 Review. Dutch.
Cited by
-
Fibrotic and emphysematous murine lung mechanics under negative-pressure ventilation.Am J Physiol Lung Cell Mol Physiol. 2025 Mar 1;328(3):L443-L455. doi: 10.1152/ajplung.00087.2024. Epub 2025 Jan 15. Am J Physiol Lung Cell Mol Physiol. 2025. PMID: 39812236 Free PMC article.
-
Positive- and Negative-Pressure Ventilation Characterized by Local and Global Pulmonary Mechanics.Am J Respir Crit Care Med. 2023 Mar 1;207(5):577-586. doi: 10.1164/rccm.202111-2480OC. Am J Respir Crit Care Med. 2023. PMID: 36194677 Free PMC article.
-
A Comparative Study of Ex-Vivo Murine Pulmonary Mechanics Under Positive- and Negative-Pressure Ventilation.Ann Biomed Eng. 2024 Feb;52(2):342-354. doi: 10.1007/s10439-023-03380-1. Epub 2023 Oct 31. Ann Biomed Eng. 2024. PMID: 37906375 Free PMC article.
-
Diaphragm Neurostimulation Assisted Ventilation in Critically Ill Patients.Am J Respir Crit Care Med. 2023 May 15;207(10):1275-1282. doi: 10.1164/rccm.202212-2252CP. Am J Respir Crit Care Med. 2023. PMID: 36917765 Free PMC article. Review.
-
Year in review 2012: Critical Care--Respirology.Crit Care. 2013 Nov 22;17(6):249. doi: 10.1186/cc13129. Crit Care. 2013. PMID: 24267541 Free PMC article. Review.
References
-
- Villar J, Blanco J, Añón JM, Santos-Bouza A, Blanch L, Ambrós A, Gandía F, Carriedo D, Mosteiro F, Basaldúa S, Fernández RL, Kacmarek RM. ALIEN Network. The ALIEN study: incidence and outcome of acute respiratory distress syndrome in the era of lung protective ventilation. Intensive Care Med. 2011;16:1932–1941. doi: 10.1007/s00134-011-2380-4. - DOI - PubMed
-
- Amato MB, Barbas CS, Medeiros DM, Magaldi RB, Schettino GP, Lorenzi-Filho G, Kairalla RA, Deheinzelin D, Munoz C, Oliveira R, Takagaki TY, Carvalho CR. Effect of a protective-ventilation strategy on mortality in the acute respiratory distress syndrome. N Engl J Med. 1998;16:347–354. doi: 10.1056/NEJM199802053380602. - DOI - PubMed
-
- The Acute Respiratory Distress Syndrome Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;16:1301–1308. - PubMed
-
- Brower RG, Lanken PN, MacIntyre N, Matthay MA, Morris A, Ancukiewicz M, Schoenfeld D, Thompson BT. National Heart, Lung, and Blood Institute ARDS Clinical Trials Network. Higher versus lower positive end-expiratory pressures in patients with the acute respiratory distress syndrome. N Engl J Med. 2004;16:327–336. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
