

Clinical findings and diagnosis in human granulocytic anaplasmosis: a case series from Massachusetts
- PMID: 22386178
- PMCID: PMC3498394
- DOI: 10.1016/j.mayocp.2011.09.008
Clinical findings and diagnosis in human granulocytic anaplasmosis: a case series from Massachusetts
Erratum in
- Mayo Clin Proc. 2012 Jun;87(6):606
Abstract
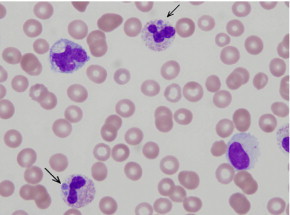
Objective: To describe clinical findings and the use of a tick-associated pathogen panel in a series of patients with human granulocytic anaplasmosis (HGA) at a suburban Boston hospital.
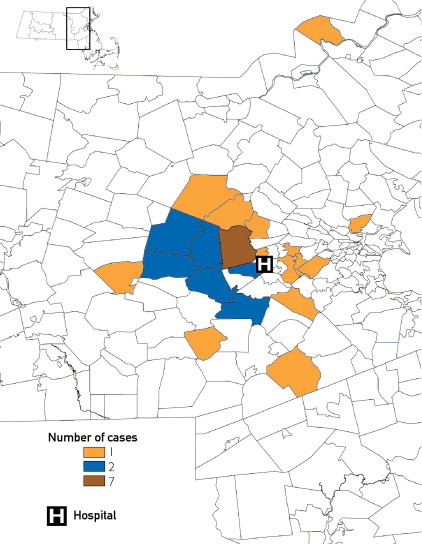
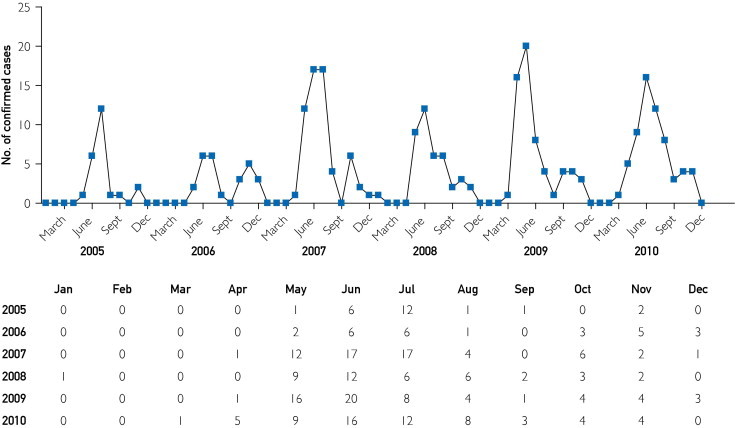
Patients and methods: Medical records were reviewed for inpatients and outpatients at Newton-Wellesley Hospital with a positive polymerase chain reaction (PCR) result for Anaplasma phagocytophilum during the study period March 1 through November 30, 2009. A PCR panel was used to test for tick-borne pathogens. Postal ZIP code data from the patients' areas of residence were used to estimate the area of disease transmission.
Results: Thirty-three cases were confirmed during the 2009 transmission season, and 14 of these patients (42%) required hospitalization. Thrombocytopenia and/or leukopenia were observed at the time of presentation in 25 of 30 patients (86%) in whom both white blood cell and platelet counts were determined, and 28 of 33 patients (85%) reported fever. Rash occurred in only 2 of the 33 patients (6%), and 25 (76%) reported one or more respiratory or gastrointestinal symptom. Cases were geographically distributed diffusely throughout the hospital catchment area, with one possible focus of infection identified in Weston, MA. Due to a lack of clinical data reporting to the Massachusetts Department of Public Health, only 20 of 32 HGA cases (63%) fulfilled the case confirmation criteria.
Conclusion: Diagnosis of HGA requires a high suspicion for infection even in endemic areas. Use of a tick-associated pathogen panel that includes PCR assays for several organisms could improve detection of underrecognized tick-borne diseases in endemic areas. Lack of epidemiological follow-up to confirm corroborating clinical findings prevents accurate case reporting and assessment of the true HGA burden.
Copyright © 2012 Mayo Foundation for Medical Education and Research. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Chapman A.S., Bakken J.S., Folk S.M., Tickborne Rickettsial Diseases Working Group; CDC Diagnosis and management of tickborne rickettsial diseases: Rocky Mountain spotted fever, ehrlichioses, and anaplasmosis—United States: a practical guide for physicians and other health-care and public health professionals. MMWR Recomm Rep. 2006;55(RR-4):1–27. - PubMed
-
- Graf P.C., Chretien J.P., Ung L., Gaydos J.C., Richards A.L. Prevalence of seropositivity to spotted fever group rickettsiae and Anaplasma phagocytophilum in a large, demographically diverse US sample. Clin Infect Dis. 2008;46(1):70–77. - PubMed
-
- Hilton E., DeVoti J., Benach J.L. Seroprevalence and seroconversion for tick-borne diseases in a high-risk population in the northeast United States. Am J Med. 1999;106(4):404–409. - PubMed
-
- Bakken J.S., Goellner P., Van Etten M. Seroprevalence of human granulocytic ehrlichiosis among permanent residents of northwestern Wisconsin. Clin Infect Dis. 1998;27(6):1491–1496. - PubMed
-
- Holden K., Boothby J.T., Anand S., Massung R.F. Detection of Borrelia burgdorferi, Ehrlichia chaffeensis, and Anaplasma phagocytophilum in ticks (Acari: Ixodidae) from a coastal region of California. J Med Entomol. 2003;40(4):534–539. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
