

Does differential drop-out explain the influence of study design on antidepressant response? A meta-analysis
- PMID: 22387053
- PMCID: PMC3586309
- DOI: 10.1016/j.jad.2012.01.031
Does differential drop-out explain the influence of study design on antidepressant response? A meta-analysis
Abstract
Background: Response to antidepressants is higher in active comparator relative to placebo-controlled clinical trials. Increased patient expectancy in comparator trials has been hypothesized to explain this finding, but previous analyses have not accounted for the increased drop-out observed in placebo-controlled trials.
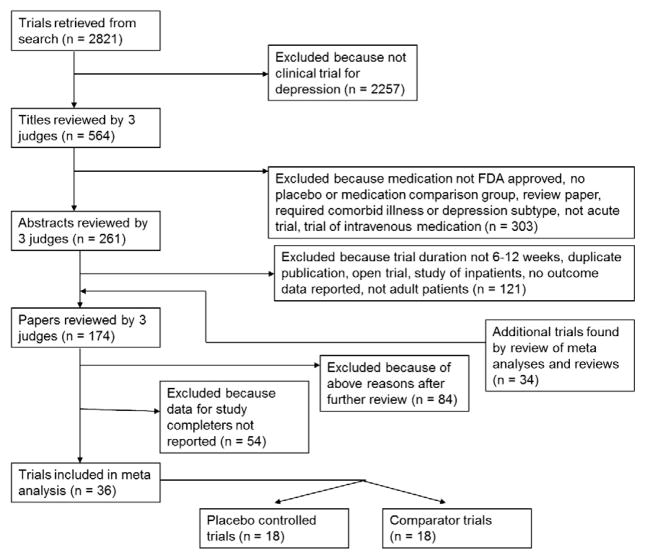
Methods: A systematic literature review was conducted to identify published antidepressant clinical trials reporting data on intent-to-treat (ITT) as well as completer patient populations. The influence of participant drop-out on observed antidepressant response was investigated by comparing the ITT and completer data sets in separate multilevel meta-analyses of antidepressant response in placebo-controlled and comparator trials.
Results: 18 placebo-controlled and 18 active comparator studies were available for analysis. Using the intent-to-treat data, the odds of responding to medication in comparator trials were 1.9 times the odds in placebo-controlled trials (95% CI=1.3-2.7, p=0.001). The same pattern was obtained among study completers, in whom the odds of responding to antidepressant medication were 1.9 times higher in comparator as opposed to placebo-controlled study designs (95% CI=1.2-3.0, p=0.009).
Limitations: Publication bias, the use of trial-level summary data, and unreported clinical or demographic differences between the ITT and completer patient populations may have influenced the study results.
Conclusions: Increased drop-out in placebo-controlled vs. active comparator studies of antidepressant medications does not appear to explain the difference in response rates between these study types. Rather, increased patient expectancy resulting from the certainty of receiving active medication in comparator trials may lead to improved response rates.
Copyright © 2012 Elsevier B.V. All rights reserved.
Conflict of interest statement
Dr. Rutherford and Dr. Sneed have no disclosures to report. Dr. Roose reports serving on a Data and Safety Monitoring Board for Medtronics, Inc. This paper has not been previously presented.
Similar articles
-
Less is more in antidepressant clinical trials: a meta-analysis of the effect of visit frequency on treatment response and dropout.J Clin Psychiatry. 2013 Jul;74(7):703-15. doi: 10.4088/JCP.12r08267. J Clin Psychiatry. 2013. PMID: 23945448 Free PMC article.
-
Design makes a difference: a meta-analysis of antidepressant response rates in placebo-controlled versus comparator trials in late-life depression.Am J Geriatr Psychiatry. 2008 Jan;16(1):65-73. doi: 10.1097/JGP.0b013e3181256b1d. Epub 2007 Nov 12. Am J Geriatr Psychiatry. 2008. PMID: 17998306 Review.
-
Drop-out rates in placebo-controlled trials of antidepressant drugs: A systematic review and meta-analysis based on clinical study reports.Int J Risk Saf Med. 2019;30(4):217-232. doi: 10.3233/JRS-195041. Int J Risk Saf Med. 2019. PMID: 31561390
-
Deconstructing pediatric depression trials: an analysis of the effects of expectancy and therapeutic contact.J Am Acad Child Adolesc Psychiatry. 2011 Aug;50(8):782-95. doi: 10.1016/j.jaac.2011.04.004. Epub 2011 Jun 15. J Am Acad Child Adolesc Psychiatry. 2011. PMID: 21784298 Free PMC article. Review.
-
Antidepressants for treating depression in dementia.Cochrane Database Syst Rev. 2018 Aug 31;8(8):CD003944. doi: 10.1002/14651858.CD003944.pub2. Cochrane Database Syst Rev. 2018. PMID: 30168578 Free PMC article.
Cited by
-
Control Group Outcomes in Trials of Psilocybin, SSRIs, or Esketamine for Depression: A Meta-Analysis.JAMA Netw Open. 2025 Jul 1;8(7):e2524119. doi: 10.1001/jamanetworkopen.2025.24119. JAMA Netw Open. 2025. PMID: 40736734 Free PMC article.
-
Clinic visits in late-life depression trials: effects on signal detection and therapeutic outcome.Am J Geriatr Psychiatry. 2014 Dec;22(12):1452-61. doi: 10.1016/j.jagp.2013.09.003. Epub 2013 Nov 5. Am J Geriatr Psychiatry. 2014. PMID: 24200597 Free PMC article.
-
Online neurocognitive remediation therapy to improve cognition in community-living individuals with a history of depression: A pilot study.Internet Interv. 2017 Apr 29;9:7-14. doi: 10.1016/j.invent.2017.04.003. eCollection 2017 Sep. Internet Interv. 2017. PMID: 30135832 Free PMC article.
-
Less is more in antidepressant clinical trials: a meta-analysis of the effect of visit frequency on treatment response and dropout.J Clin Psychiatry. 2013 Jul;74(7):703-15. doi: 10.4088/JCP.12r08267. J Clin Psychiatry. 2013. PMID: 23945448 Free PMC article.
-
Comparative efficacy and acceptability of first-generation and second-generation antidepressants in the acute treatment of major depression: protocol for a network meta-analysis.BMJ Open. 2016 Jul 8;6(7):e010919. doi: 10.1136/bmjopen-2015-010919. BMJ Open. 2016. PMID: 27401359 Free PMC article.
References
-
- Alves C, Cachola I, Brandao J. Efficacy and tolerability of venlafaxine and fluoxetine in outpatients with major depression. Primary Care Psychiatry. 1999;5:57–63.
-
- Baldwin DS, Hawley CJ, et al. A multicenter double-blind comparison of nefazodone and paroxetine in the treatment of outpatients with moderate-to-severe depression. The Journal of Clinical Psychiatry. 1996;57 (Suppl 2):46–52. - PubMed
-
- Beck AT, Ward CH, Mendelson M, et al. An inventory of measuring depression. Archives of General Psychiatry. 1961;4:53–63. - PubMed
-
- Benkert O, Szegedi A, et al. Mirtazapine compared with paroxetine in major depression. The Journal of Clinical Psychiatry. 2000;61:656–663. - PubMed
-
- Birge RT. The calculation of errors by the method of least squares. Reviews of Modern Physics. 1932;40:207–227.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
