

Trocar-assisted sutureless intrascleral posterior chamber foldable intra-ocular lens fixation
- PMID: 22388599
- PMCID: PMC3376277
- DOI: 10.1038/eye.2012.19
Trocar-assisted sutureless intrascleral posterior chamber foldable intra-ocular lens fixation
Abstract
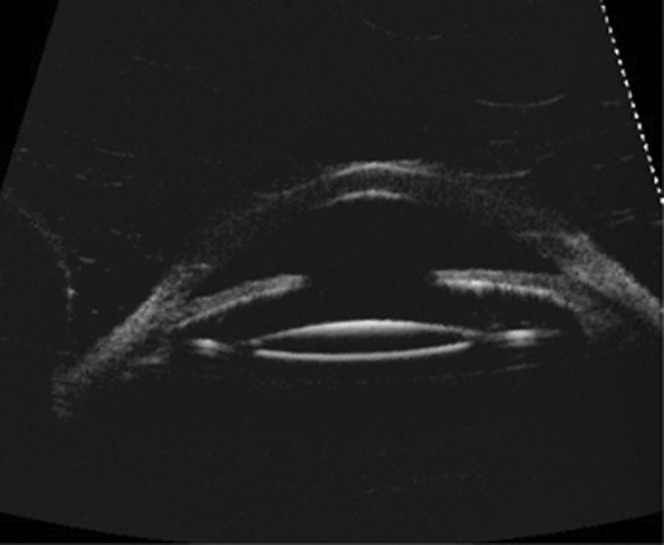
Purpose: We report a novel technique characterized by sutureless scleral fixation of three-pieces foldable intraocular lens (IOL) using 25-gauge transconjunctival sutureless vitrectomy (TSV) trocars in patients with insufficient posterior capsule support.
Materials and methods: We performed this technique on the eight eyes of the seven patients. The scleral tunnels (STs) are prepared by insertion of the 25-gauge TSV microcannulas using the trocars, and anterior vitrectomy is performed through the clear corneal paracentesis with the aid of anterior chamber maintainer (ACM). Finally, the three-piece foldable IOL haptics are incarcerated into the prepared STs.
Results: The patients were followed up 5-8 months. None of the patients had complications such as postoperative endophthalmitis, glaucoma, IOL tilt or decentralization, and retinal detachment. Injection of a foldable IOL through a clear corneal small incision also contributes the less surgical-induced astigmatism.
Conclusion: The presented novel sutureless scleral IOL fixation technique may provide minimal trauma to the surrounding tissues, good IOL stabilization decreasing the incidence of IOL tilt along with shorter operation time, and postoperative quiet eye.
Figures





References
-
- Smiddy WE. Dislocated posterior chamber intraocular lens; a new technique of management. Arch Ophthalmol. 1989;107:1678–1680. - PubMed
-
- Nabors G, Varley MP, Charles S. Ciliary sulcus suturing of a posterior chamber intraocular lens. Ophthalmic Surg. 1990;21:263–265. - PubMed
-
- Azar DT, Wiley WF. Double-knot transscleral suture fixation technique for displaced intraocular lenses. Am J Ophthalmol. 1999;128:644–646. - PubMed
-
- Baykara M, Ozcetin H, Yilmaz S, Timuçin OB. Posterior iris fixation of the iris-claw intraocular lens implantation through a scleral tunnel incision. Am J Ophthalmol. 2007;144:586–591. - PubMed
-
- Dick HB, Augustin AJ. Lens implant selection with absence of capsular support. Curr Opin Ophthalmol. 2001;12:47–57. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
