

Early appearance of neutralizing immunoglobulin G3 antibodies is associated with chikungunya virus clearance and long-term clinical protection
- PMID: 22389226
- PMCID: PMC3295607
- DOI: 10.1093/infdis/jis033
Early appearance of neutralizing immunoglobulin G3 antibodies is associated with chikungunya virus clearance and long-term clinical protection
Abstract
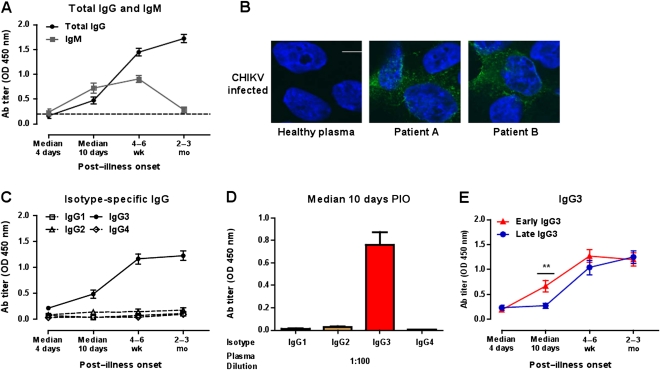
Background: Chikungunya virus (CHIKV) and related arboviruses have been responsible for large epidemic outbreaks with serious economic and social impact. Although infected individuals clear the virus from the blood, some develop debilitating and prolonged arthralgia.
Methods: We investigated specificity and strength of antibody responses in a longitudinal study on CHIKV-infected patients and analyzed their association with viral load, cytokine profile, and severity.
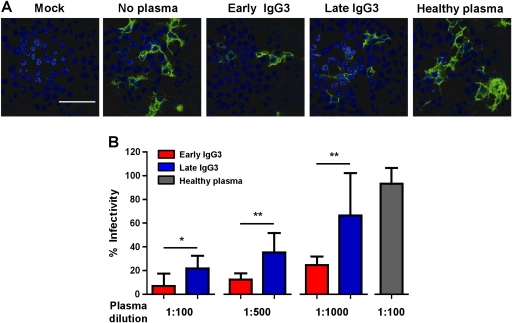
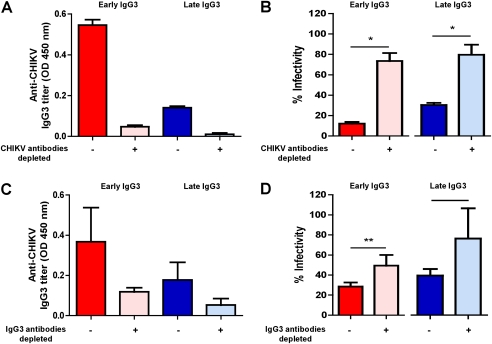
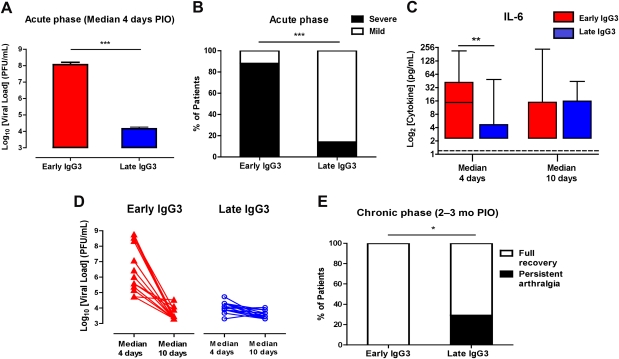
Results: We found that CHIKV-specific response is dominated by immunoglobulin G3 (IgG3) antibodies. The antibodies were neutralizing, and patients with high viremia rapidly developed high levels of anti-CHIKV antibodies of this specific isotype. Although these patients endured a more severe disease progression during the acute viremic phase, they cleared the virus faster and did not experience persistent arthralgia. However, significant persistent arthralgia was observed in patients with low viremia who developed IgG3 at a later stage.
Conclusions: Absence of early CHIKV-specific IgG3 may therefore serve as a specific marker of patients with increased risk of disease.
Figures
References
-
- Powers AM, Logue CH. Changing patterns of chikungunya virus: re-emergence of a zoonotic arbovirus. J Gen Virol. 2007;88:2363–77. - PubMed
-
- Higgs S. The 2005–2006 chikungunya epidemic in the Indian Ocean. Vector Borne Zoonotic Dis. 2006;6:115–6. - PubMed
-
- Lumsden WH. An epidemic of virus disease in Southern Province, Tanganyika Territory, in 1952–53. II. General description and epidemiology. Trans R Soc Trop Med Hyg. 1955;49:33–57. - PubMed
-
- Robinson MC. An epidemic of virus disease in Southern Province, Tanganyika Territory, in 1952–53. I. Clinical features. Trans R Soc Trop Med Hyg. 1955;49:28–32. - PubMed
-
- Kondekar S, Gogtay NJ. Why chikungunya is called chikungunya. J Post Med. 2006;52:307.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
