

Intervention strategies to reduce the burden of non-communicable diseases in Mexico: cost effectiveness analysis
- PMID: 22389335
- PMCID: PMC3292518
- DOI: 10.1136/bmj.e355
Intervention strategies to reduce the burden of non-communicable diseases in Mexico: cost effectiveness analysis
Abstract
Objective: To inform decision making regarding intervention strategies against non-communicable diseases in Mexico, in the context of health reform.
Design: Cost effectiveness analysis based on epidemiological modelling.
Interventions: 101 intervention strategies relating to nine major clusters of non-communicable disease: depression, heavy alcohol use, tobacco use, cataracts, breast cancer, cervical cancer, chronic obstructive pulmonary disease, cardiovascular disease, and diabetes.
Data sources: Mexican data sources were used for most key input parameters, including administrative registries; disease burden and population estimates; household surveys; and drug price databases. These sources were supplemented as needed with estimates for Mexico from the WHO-CHOICE unit cost database or with estimates extrapolated from the published literature.
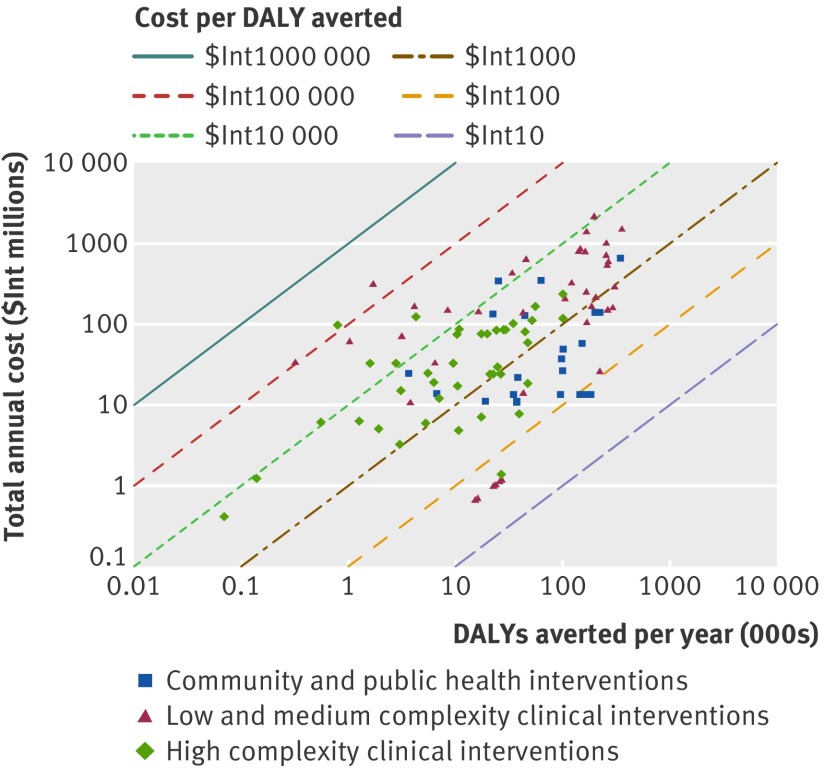
Main outcome measures: Population health outcomes, measured in disability adjusted life years (DALYs); costs in 2005 international dollars ($Int); and costs per DALY.
Results: Across 101 intervention strategies examined in this study, average yearly costs at the population level would range from around ≤$Int1m (such as for cataract surgeries) to >$Int1bn for certain strategies for primary prevention in cardiovascular disease. Wide variation also appeared in total population health benefits, from <1000 DALYs averted a year (for some components of cancer treatments or aspirin for acute ischaemic stroke) to >300,000 averted DALYs (for aggressive combinations of interventions to deal with alcohol use or cardiovascular risks). Interventions in this study spanned a wide range of average cost effectiveness ratios, differing by more than three orders of magnitude between the lowest and highest ratios. Overall, community and public health interventions such as non-personal interventions for alcohol use, tobacco use, and cardiovascular risks tended to have lower cost effectiveness ratios than many clinical interventions (of varying complexity). Even within the community and public health interventions, however, there was a 200-fold difference between the most and least cost effective strategies examined. Likewise, several clinical interventions appeared among the strategies with the lowest average cost effectiveness ratios-for example, cataract surgeries.
Conclusions: Wide variations in costs and effects exist within and across intervention categories. For every major disease area examined, at least some strategies provided excellent value for money, including both population based and personal interventions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
References
-
- Frenk J, Gonzalez-Pier E, Gomez-Dantes O, Lezana MA, Knaul FM. Comprehensive reform to improve health system performance in Mexico. Lancet 2006;368:1524-34. - PubMed
-
- Secretaría de Hacienda y Crédito Público. Presupuesto de Egresos de la Federación. http://shcp.gob.mx/EGRESOS/PEF/Paginas/PresupuestodeEgresos.aspx.
-
- Comisión Nacional de Protección Social en Salud. Sistema de Protección Social en Salud: Informe de Resultados 2010. Secretaria de Salud, 2011.
-
- Gonzalez-Pier E, Gutierrez-Delgado C, Stevens G, Barraza-Llorens M, Porras-Condey R, Carvalho N, et al. Priority setting for health interventions in Mexico’s System of Social Protection in Health. Lancet 2006;368:1608-18. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources