

Cost effectiveness of strategies to combat vision and hearing loss in sub-Saharan Africa and South East Asia: mathematical modelling study
- PMID: 22389341
- PMCID: PMC3292524
- DOI: 10.1136/bmj.e615
Cost effectiveness of strategies to combat vision and hearing loss in sub-Saharan Africa and South East Asia: mathematical modelling study
Abstract
Objective: To determine the relative costs, effects, and cost effectiveness of selected interventions to control cataract, trachoma, refractive error, hearing loss, meningitis and chronic otitis media.
Design: Cost effectiveness analysis of or combined strategies for controlling vision and hearing loss by means of a lifetime population model.
Setting: Two World Health Organization sub-regions of the world where vision and hearing loss are major burdens: sub-Saharan Africa and South East Asia.
Data sources: Biological and behavioural parameters from clinical and observational studies and population based surveys. Intervention effects and resource inputs based on published reports, expert opinion, and the WHO-CHOICE database.
Main outcome measures: Cost per disability adjusted life year (DALY) averted, expressed in international dollars ($Int) for the year 2005.
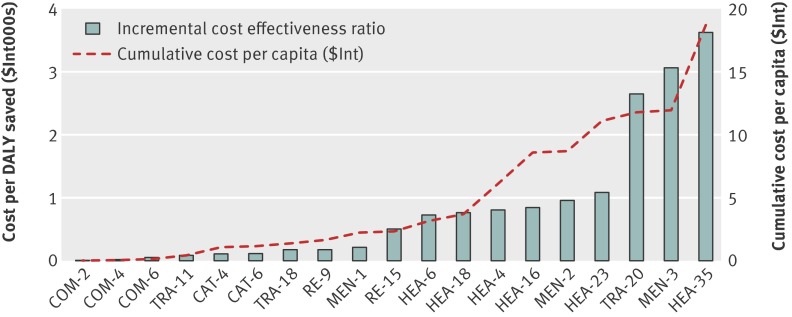
Results: Treatment of chronic otitis media, extracapsular cataract surgery, trichiasis surgery, treatment for meningitis, and annual screening of schoolchildren for refractive error are among the most cost effective interventions to control hearing and vision impairment, with the cost per DALY averted <$Int285 in both regions. Screening of both schoolchildren (annually) and adults (every five years) for hearing loss costs around $Int1000 per DALY averted. These interventions can be considered highly cost effective. Mass treatment with azithromycin to control trachoma can be considered cost effective in the African but not the South East Asian sub-region.
Conclusions: Vision and hearing impairment control interventions are generally cost effective. To decide whether substantial investments in these interventions is warranted, this finding should be considered in relation to the economic attractiveness of other, existing or new, interventions in health.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures
References
-
- World Health Organization. Fact sheet—magnitude and causes of visual impairment. WHO, 2011. www.who.int/mediacentre/factsheets/fs282/en/.
-
- Mathers C, Smith A, Concha M. Global burden of hearing loss in the year 2000. WHO, 2002. www.who.int/healthinfo/statistics/bod_hearingloss.pdf .
-
- Mathers C, Smith A, Concha M. Global burden of adult-onset hearing loss in the year 2002. WHO, 2005.
-
- Smith A, Mathers C. Epidemiology of infection as a cause of hearing loss. In: Newton VE, Vallely PJ, eds. Infection and hearing impairment. John Wiley, 2006.
-
- Mackenzie I, Smith A. Deafness—the neglected and hidden disability. Ann Trop Med Parasitol 2009;103:565-71. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical