

Differentiating among incretin-based therapies in the management of patients with type 2 diabetes mellitus
- PMID: 22390369
- PMCID: PMC3310739
- DOI: 10.1186/1758-5996-4-8
Differentiating among incretin-based therapies in the management of patients with type 2 diabetes mellitus
Abstract
The glucagon-like peptide-1 receptor (GLP-1R) agonists and dipeptidyl peptidase-4 (DPP-4) inhibitors have become important options for the management of patients with type 2 diabetes mellitus. While the GLP-1R agonists and DPP-4 inhibitors act on the incretin system to regulate glucose homeostasis, there are important clinical differences among the five agents currently available in the U.S. For example, the GLP-1R agonists require subcutaneous administration, produce pharmacological levels of GLP-1 activity, promote weight loss, have a more robust glucose-lowering effect, and have a higher incidence of adverse gastrointestinal effects. In contrast, the DPP-4 inhibitors are taken orally, increase the half-life of endogenous GLP-1, are weight neutral, and are more commonly associated with nasopharyngitis. Differences in efficacy, safety, tolerability, and cost among the incretin-based therapies are important to consider in the primary care management of patients with type 2 diabetes mellitus.
Figures

Similar articles
-
The pharmacologic basis for clinical differences among GLP-1 receptor agonists and DPP-4 inhibitors.Postgrad Med. 2011 Nov;123(6):189-201. doi: 10.3810/pgm.2011.11.2508. Postgrad Med. 2011. PMID: 22104467
-
Glycaemic efficacy of glucagon-like peptide-1 receptor agonists and dipeptidyl peptidase-4 inhibitors as add-on therapy to metformin in subjects with type 2 diabetes-a review and meta analysis.Diabetes Obes Metab. 2012 Aug;14(8):762-7. doi: 10.1111/j.1463-1326.2012.01603.x. Epub 2012 Apr 24. Diabetes Obes Metab. 2012. PMID: 22471248 Review.
-
Cardiovascular Actions and Clinical Outcomes With Glucagon-Like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors.Circulation. 2017 Aug 29;136(9):849-870. doi: 10.1161/CIRCULATIONAHA.117.028136. Circulation. 2017. PMID: 28847797 Review.
-
Enhancing incretin action for the treatment of type 2 diabetes.Diabetes Care. 2003 Oct;26(10):2929-40. doi: 10.2337/diacare.26.10.2929. Diabetes Care. 2003. PMID: 14514604 Review.
-
An updated review on cancer risk associated with incretin mimetics and enhancers.J Environ Sci Health C Environ Carcinog Ecotoxicol Rev. 2015;33(1):67-124. doi: 10.1080/10590501.2015.1003496. J Environ Sci Health C Environ Carcinog Ecotoxicol Rev. 2015. PMID: 25803196 Review.
Cited by
-
Use of Canagliflozin in Combination With and Compared to Incretin-Based Therapies in Type 2 Diabetes.Clin Diabetes. 2017 Jul;35(3):141-153. doi: 10.2337/cd16-0063. Clin Diabetes. 2017. PMID: 28761216 Free PMC article.
-
Sitagliptin reduces cardiac apoptosis, hypertrophy and fibrosis primarily by insulin-dependent mechanisms in experimental type-II diabetes. Potential roles of GLP-1 isoforms.PLoS One. 2013 Oct 21;8(10):e78330. doi: 10.1371/journal.pone.0078330. eCollection 2013. PLoS One. 2013. PMID: 24302978 Free PMC article.
-
Diabetes-related alterations in the enteric nervous system and its microenvironment.World J Diabetes. 2012 May 15;3(5):80-93. doi: 10.4239/wjd.v3.i5.80. World J Diabetes. 2012. PMID: 22645637 Free PMC article.
-
Efficacy and tolerability of GLP-1 agonists in patients with type 2 diabetes mellitus: an Indian perspective.Ther Adv Endocrinol Metab. 2014 Dec;5(6):159-65. doi: 10.1177/2042018814552657. Ther Adv Endocrinol Metab. 2014. PMID: 25489471 Free PMC article. Review.
-
A review of glycemic efficacy of liraglutide once daily in achieving glycated hemoglobin targets compared with exenatide twice daily, or sitagliptin once daily in the treatment of type 2 diabetes.Saudi Med J. 2016 Aug;37(8):834-42. doi: 10.15537/smj.2016.8.15800. Saudi Med J. 2016. PMID: 27464858 Free PMC article. Review.
References
-
- Skyler JS, Bergenstal R, Bonow RO, Buse J, Deedwania P, Gale EA, Howard BV, Kirkman MS, Kosiborod M, Reaven P, Sherwin RS. Intensive glycemic control and the prevention of cardiovascular events: implications of the ACCORD, ADVANCE, and VA diabetes trials: a position statement of the American Diabetes Association and a scientific statement of the American College of Cardiology Foundation and the American Heart Association. Circulation. 2009;119:351–357. doi: 10.1161/CIRCULATIONAHA.108.191305. - DOI - PubMed
-
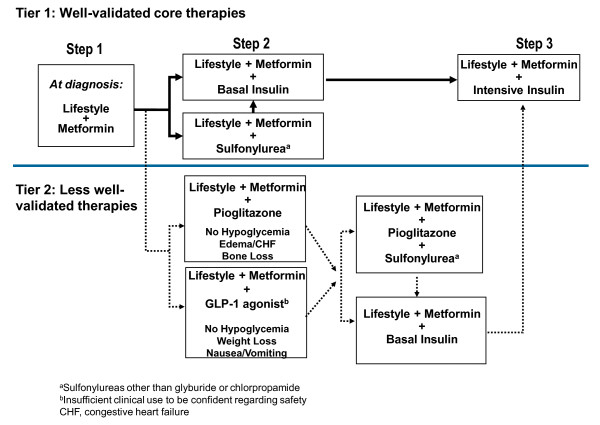
- Nathan DM, Buse JB, Davidson MB, Ferrannini E, Holman RR, Sherwin R, Zinman B. Medical management of hyperglycemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy: a consensus statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2009;32:193–203. doi: 10.2337/dc08-9025. - DOI - PMC - PubMed
-
- Rodbard HW, Jellinger PS, Davidson JA, Einhorn D, Garber AJ, Grunberger G, Handelsman Y, Horton ES, Lebovitz H, Levy P, Moghissi ES, Schwartz SS. Statement by an American Association of Clinical Endocrinologists/American College of Endocrinology consensus panel on type 2 diabetes mellitus: an algorithm for glycemic control. Endocr Pract. 2009;15:540–559. - PubMed
-
- Nauck MA. Unraveling the science of incretin biology. Am J Med. 2009;122:S3–S10. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
