

Episiotomy characteristics and risks for obstetric anal sphincter injuries: a case-control study
- PMID: 22390647
- PMCID: PMC3489037
- DOI: 10.1111/j.1471-0528.2012.03293.x
Episiotomy characteristics and risks for obstetric anal sphincter injuries: a case-control study
Abstract
Objectives: To investigate the association between the geometrical properties of episiotomy and obstetric anal sphincter injuries (OASIS) because episiotomies angled at 40-60° are associated with fewer OASIS than episiotomies with more acute angles.
Design: Case-control study.
Setting: University Hospital of North Norway, Tromsø and Nordland Hospital, Bodø, Norway.
Sample: Seventy-four women who had one vaginal birth and episiotomy. Cases (n = 37) have sustained OASIS at birth, while controls (n = 37) had not. The groups were matched for instrumental delivery.
Methods: Two groups of women with history of only one vaginal birth were compared. Episiotomy scar was identified and photographed and relevant measures were taken. Data were analysed using conditional logistic analysis.
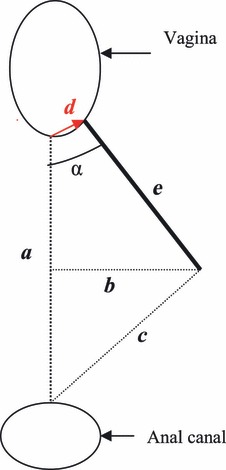
Main outcome measures: Mean episiotomy angle, length, depth, incision point.
Results: The risk of sustaining OASIS decreased by 70% (odds ratio [OR] 0.30; 95% CI 0.14-0.66) for each 5.5-mm increase in episiotomy depth, decreased by 56% (OR 0.44; 95% CI 0.23-0.86) for each 4.5-mm increase in the distance from the midline to the incision point of the episiotomy, and decreased by 75% (OR 0.25; 95% CI 0.10-0.61) for each 5.5-mm increase in episiotomy length. Lastly, there was no difference in mean angle between groups but there was a "U-shaped" association between angle and OASIS (OR 2.09; 95% CI 1.02-4.28) with an increased risk (OR 9.00; 95% CI 1.1-71.0) of OASIS when the angle was either smaller than 15° or >60°.
Conclusion: The present study showed that scarred episiotomies with depth > 16 mm, length > 17 mm, incision point > 9 mm lateral of midpoint and angle range 30-60° are significantly associated with less risk of OASIS. Shrinkage of tissue must be considered.
© 2012 The Authors BJOG An International Journal of Obstetrics and Gynaecology © 2012 RCOG.
Figures

Comment in
-
Episiotomy characteristics and risks for obstetric anal sphincter injuries: a case-control study.BJOG. 2012 Aug;119(9):1147; author reply 1148-9. doi: 10.1111/j.1471-0528.2012.03390.x. BJOG. 2012. PMID: 22780819 No abstract available.
-
Avoiding episiotomy is the best strategy to prevent OASIS: response to the article 'episiotomy characteristics and risks for obstetric anal sphincter injuries: a case-control study'.BJOG. 2012 Aug;119(9):1148; author reply 1148-9. doi: 10.1111/j.1471-0528.2012.03391.x. BJOG. 2012. PMID: 22780821 No abstract available.
References
-
- Norderval S, Nsubuga D, Bjelke C, Frasunek J, Myklebust I, Vonen B. Anal incontinence after obstetric sphincter tears: incidence in a Norwegian county. Acta Obstet Gynecol Scand. 2004;83:989–94. - PubMed
-
- Roos AM, Thakar MR, Sultan MA. Outcome of primary repair of obstetric anal sphincter injuries (OASIS)—does the grade of tear matter? Ultrasound Obstet Gynecol. 2009;36:368–7. - PubMed
-
- Dudding TC, Vaizey CJ, Kamm MA. Obstetric anal sphincter injury: incidence, risk factors, and management. Ann Surg. 2008;247:224–37. - PubMed
-
- Hartmann K, Viswanathan M, Palmieri R, Gartlehner G, Thorp J, Jr, Lohr KN. Outcomes of routine episiotomy: a systematic review. JAMA. 2005;293:2141–8. - PubMed
