

Primary screening for human papillomavirus compared with cytology screening for cervical cancer in European settings: cost effectiveness analysis based on a Dutch microsimulation model
- PMID: 22391612
- PMCID: PMC3293782
- DOI: 10.1136/bmj.e670
Primary screening for human papillomavirus compared with cytology screening for cervical cancer in European settings: cost effectiveness analysis based on a Dutch microsimulation model
Abstract
Objectives: To investigate, using a Dutch model, whether and under what variables framed for other European countries screening for human papillomavirus (HPV) is preferred over cytology screening for cervical cancer, and to calculate the preferred number of examinations over a woman's lifetime.
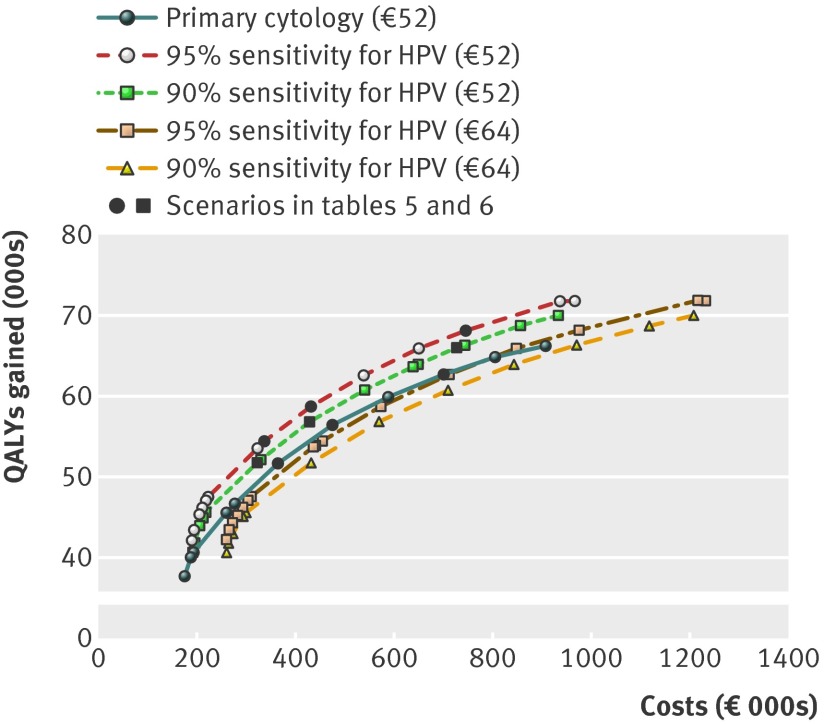
Design: Cost effectiveness analysis based on a Dutch simulation model. Base case analyses investigated the cost effectiveness of more than 1500 different screening policies using the microsimulation model. Subsequently, the policies were compared for five different scenarios that represent different possible scenarios (risk of cervical cancer, previous screening, quality associated test characteristics, costs of testing, and prevalence of HPV).
Setting: Various European countries.
Population: Unvaccinated women born between 1939 and 1992.
Main outcome measures: Optimal screening strategy in terms of incremental cost effectiveness ratios (costs per quality adjusted life years gained) compared with different cost effectiveness thresholds, for two levels of sensitivity and costs of the HPV test.
Results: Primary HPV screening was the preferred primary test over the age of 30 in many considered scenarios. Primary cytology screening was preferred only in scenarios with low costs of cytology and in scenarios with a high prevalence of HPV in combination with high costs of HPV testing.
Conclusions: Most European countries should consider switching from primary cytology to HPV screening for cervical cancer. HPV screening must, however, only be implemented in situations where screening is well controlled.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
European cost-effectiveness analysis of cervical screening strategies for women not vaccinated for HPV: in many scenarios primary HPV screening is preferable to primary cytology screening in women aged over 30 years.Evid Based Nurs. 2013 Jan;16(1):8-9. doi: 10.1136/eb-2012-100774. Epub 2012 Sep 28. Evid Based Nurs. 2013. PMID: 23024211 No abstract available.
References
-
- Bray F, Loos AH, McCarron P, Weiderpass E, Arbyn M, Moller H, et al. Trends in cervical squamous cell carcinoma incidence in 13 European countries: changing risk and the effects of screening. Cancer Epidemiol Biomarkers Prev 2005;14:677-86. - PubMed
-
- Karim-Kos HE, de Vries E, Soerjomataram I, Lemmens V, Siesling S, Coebergh JW. Recent trends of cancer in Europe: a combined approach of incidence, survival and mortality for 17 cancer sites since the 1990s. Eur J Cancer 2008;44:1345-89. - PubMed
-
- Arbyn M, Raifu AO, Weiderpass E, Bray F, Anttila A. Trends of cervical cancer mortality in the member states of the European Union. Eur J Cancer 2009;45:2640-8. - PubMed
-
- Arbyn M, Raifu AO, Autier P, Ferlay J. Burden of cervical cancer in Europe: estimates for 2004. Ann Oncol 2007;18:1708-15. - PubMed
-
- Levy-Bruhl D, Bousquet V, King LA, O’Flanagan D, Bacci S, Lopalco PL, et al. The current state of introduction of HPV vaccination into national immunisation schedules in Europe: results of the VENICE 2008 survey. Eur J Cancer 2009;45:2709-13. - PubMed