

Multidose optimization simulation of erythropoietin treatment in preterm infants
- PMID: 22391632
- PMCID: PMC3564226
- DOI: 10.1038/pr.2011.75
Multidose optimization simulation of erythropoietin treatment in preterm infants
Abstract
Introduction: Preterm infants commonly develop anemia requiring red blood cell transfusions (RBCTx). Although an alternative therapy is recombinant human erythropoietin (Epo), it is not widely employed. To provide a rigorous scientific basis supporting the latter approach, a model-based simulation analysis of endogenous erythropoiesis was developed.
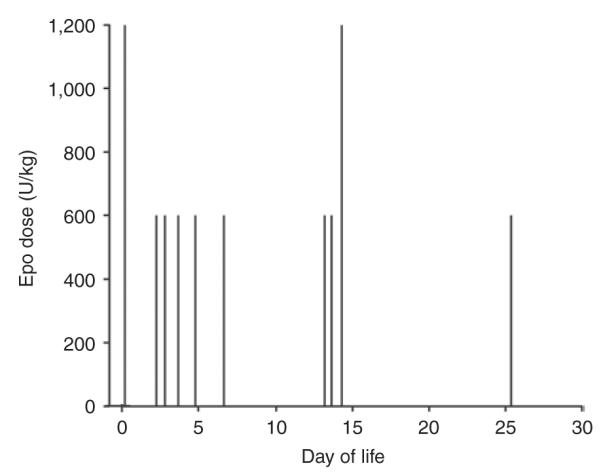
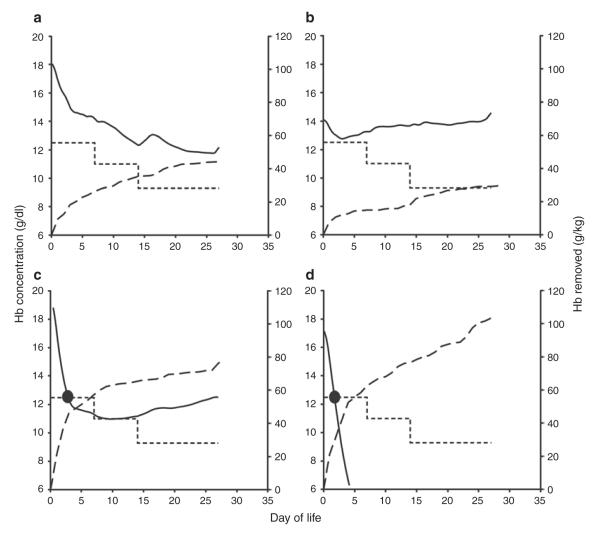
Results: The pharmacodynamic/pharmacokinetic (PK/PD) model identified an optimal Epo dosing algorithm in preterm infants that demonstrated maximal efficacy when Epo was dosed frequently during the early weeks of life (when phlebotomy loss is greatest). Model-based simulations employing optimized Epo dosing predicted that 13 of the 27 (46%) infants would avoid RBCTx ("good responders"). Importantly, simulation results identified five subject-specific covariate factors predictive of good Epo response.
Discussion: This simulation study provides a basis for possibly eliminating RBCTx in infants who can be selected for optimized Epo therapy.
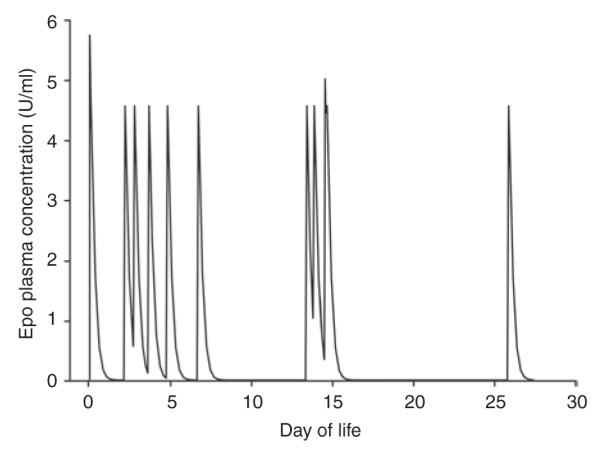
Methods: Epo PD hemoglobin production parameters were determined in 27 preterm infants studied intensively during the first 28 d of life. Model-derived Epo PD parameters were combined with PK parameters derived from the literature to simulate an optimized intravenous Epo bolus dosing schedule. The goal of this simulated optimized schedule was to eliminate RBCTx, as prescribed per current guidelines, in as many preterm infants as possible.
Figures
References
-
- Strauss RG. Red blood cell transfusion practices in the neonate. Clin Perinatol. 1995;22:641–55. - PubMed
-
- Madan A, Kumar R, Adams MM, Benitz WE, Geaghan SM, Widness JA. Reduction in red blood cell transfusions using a bedside analyzer in extremely low birth weight infants. J Perinatol. 2005;25:21–5. - PubMed
-
- Widness JA, Veng-Pedersen P, Peters C, Pereira LM, Schmidt RL, Lowe LS. Erythropoietin pharmacokinetics in premature infants: developmental, nonlinearity, and treatment effects. J Appl Physiol. 1996;80:140–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
