

Inhibition of epidermal growth factor receptor tyrosine kinase ameliorates collagen-induced arthritis
- PMID: 22393153
- PMCID: PMC3311775
- DOI: 10.4049/jimmunol.1102693
Inhibition of epidermal growth factor receptor tyrosine kinase ameliorates collagen-induced arthritis
Abstract
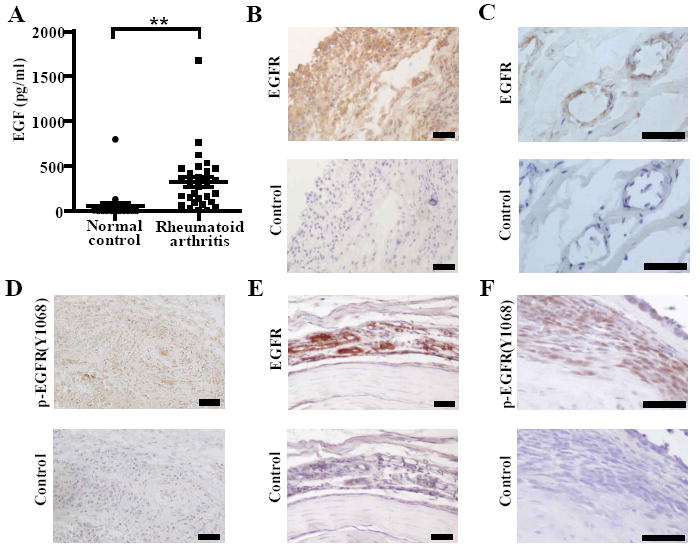
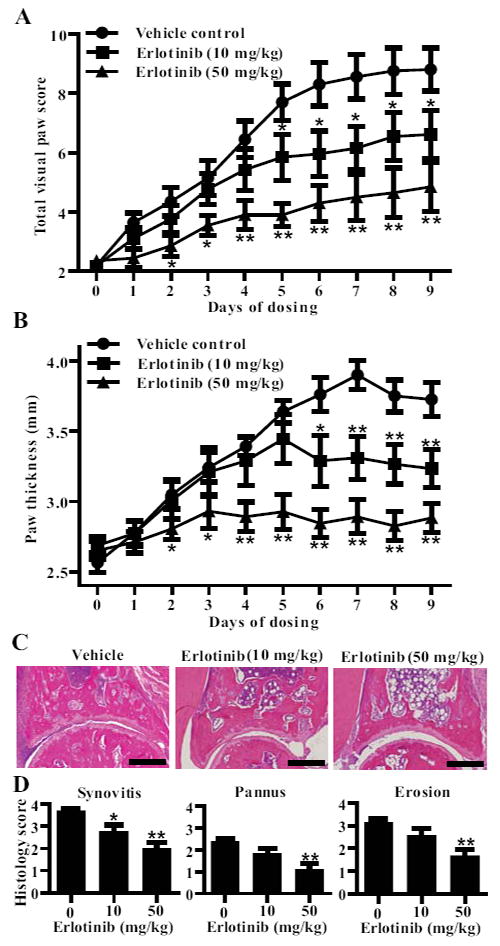
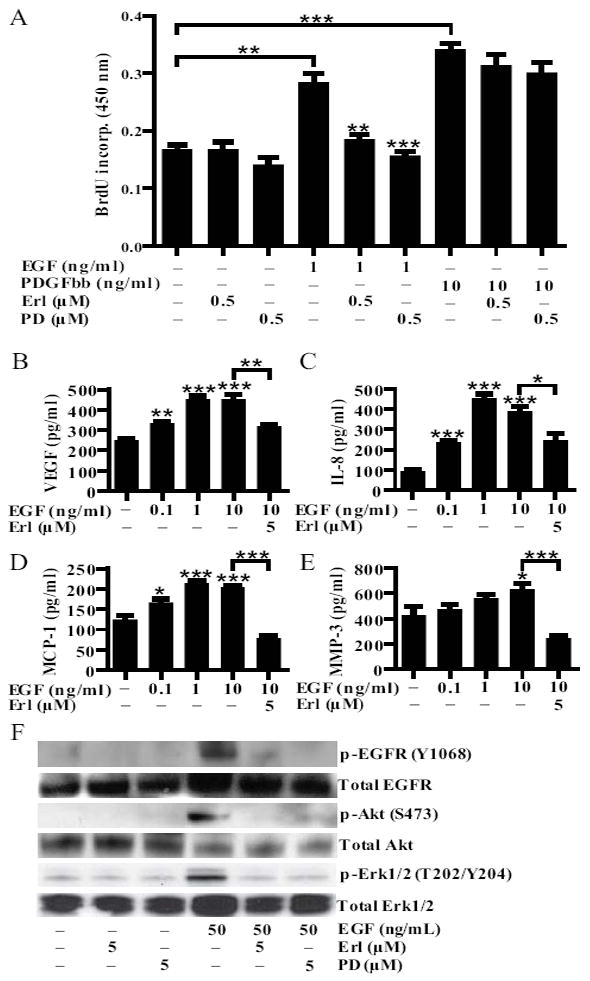
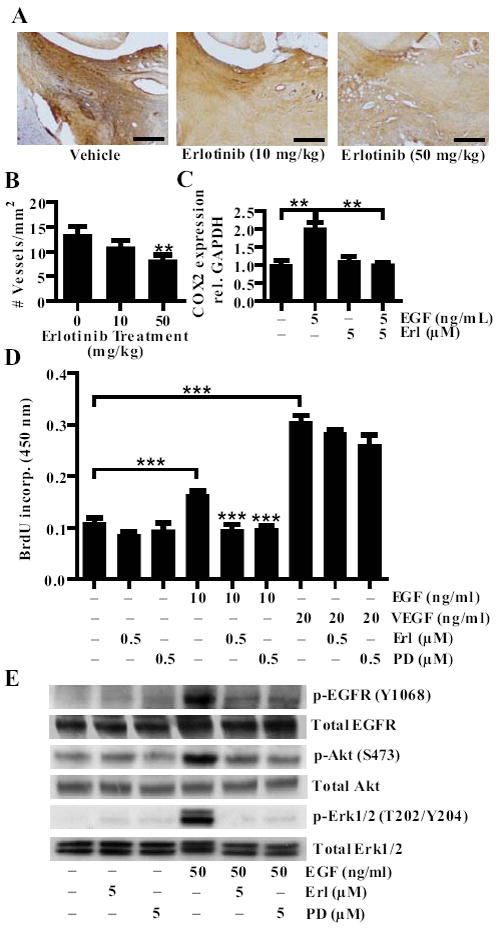
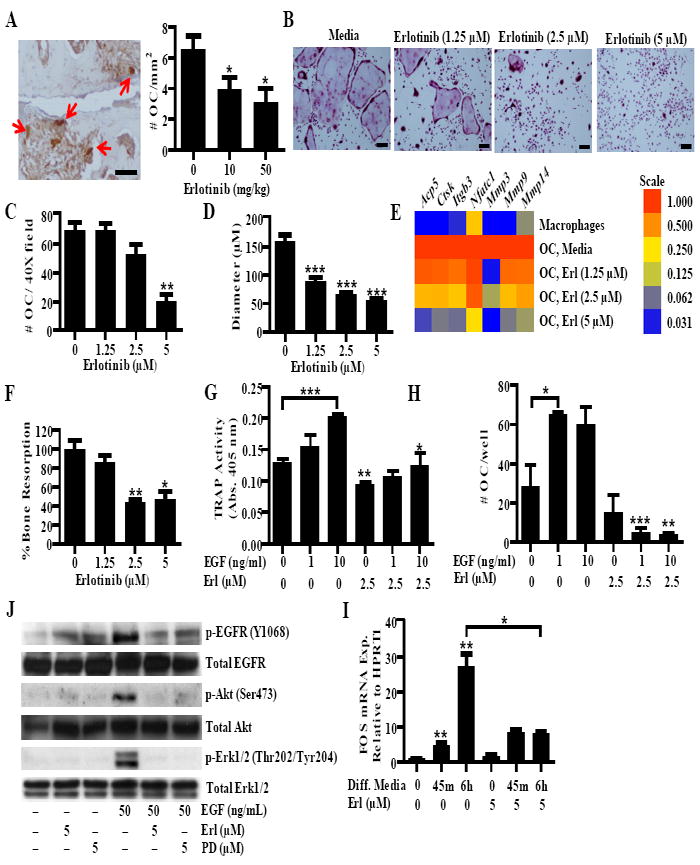
Rheumatoid arthritis (RA) is an autoimmune synovitis characterized by the formation of pannus and the destruction of cartilage and bone in the synovial joints. Although immune cells, which infiltrate the pannus and promote inflammation, play a prominent role in the pathogenesis of RA, other cell types also contribute. Proliferation of synovial fibroblasts, for example, underlies the formation of the pannus, while proliferation of endothelial cells results in neovascularization, which supports the growth of the pannus by supplying it with nutrients and oxygen. The synovial fibroblasts also promote inflammation in the synovium by producing cytokines and chemokines. Finally, osteoclasts cause the destruction of bone. In this study, we show that erlotinib, an inhibitor of the tyrosine kinase epidermal growth factor receptor (EGFR), reduces the severity of established collagen-induced arthritis, a mouse model of RA, and that it does so by targeting synovial fibroblasts, endothelial cells, and osteoclasts. Erlotinib-induced attenuation of autoimmune arthritis was associated with a reduction in number of osteoclasts and blood vessels, and erlotinib inhibited the formation of murine osteoclasts and the proliferation of human endothelial cells in vitro. Erlotinib also inhibited the proliferation and cytokine production of human synovial fibroblasts in vitro. Moreover, EGFR was highly expressed and activated in the synovium of mice with collagen-induced arthritis and patients with RA. Taken together, these findings suggest that EGFR plays a central role in the pathogenesis of RA and that EGFR inhibition may provide benefits in the treatment of RA.
Figures
Comment in
-
Experimental arthritis: Targeting EGFR to fight synovitis.Nat Rev Rheumatol. 2012 Mar 27;8(5):247. doi: 10.1038/nrrheum.2012.45. Nat Rev Rheumatol. 2012. PMID: 22450555 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
