

Point-of-care test for detection of urogenital chlamydia in women shows low sensitivity. A performance evaluation study in two clinics in Suriname
- PMID: 22393383
- PMCID: PMC3290553
- DOI: 10.1371/journal.pone.0032122
Point-of-care test for detection of urogenital chlamydia in women shows low sensitivity. A performance evaluation study in two clinics in Suriname
Abstract
Background: In general, point-of-care (POC) tests for Chlamydia trachomatis (Ct) show disappointing test performance, especially disappointing sensitivity results. However, one study sponsored by the manufacturer (Diagnostics for the Real World) reported over 80% sensitivity with their Chlamydia Rapid Test (CRT). We evaluated the performance of this CRT in a non-manufacturer-sponsored trial.
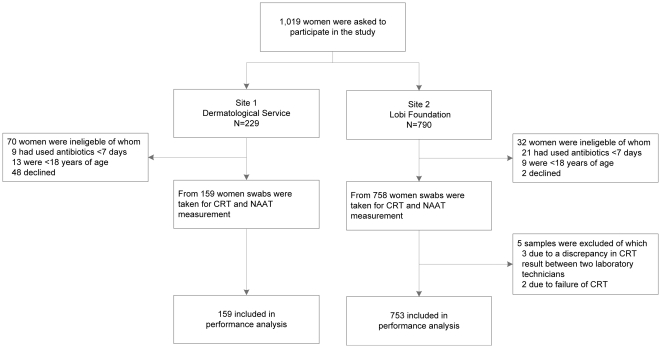
Methods: Between July 2009 and February 2010, we included samples from 912 women in both high- and low-risk clinics for sexually transmitted infections (STIs) in Paramaribo, Suriname. Sensitivity, specificity, positive- and negative predictive values (PPV and NPV) for CRT compared to NAAT (Aptima, Gen-Probe) were determined. Quantitative Ct load and human cell load were determined in all CRT and/or NAAT positive samples.
Results: CRT compared to NAAT showed a sensitivity and specificity of 41.2% (95% CI, 31.9%-50.9%) and 96.4% (95% CI, 95.0%-97.5%), respectively. PPV and NPV were 59.2% (95% CI, 47.5%-70.1%) and 92.9% (95% CI, 91.0%-94.5%), respectively. Quantitative Ct bacterial load was 73 times higher in NAAT-positive/CRT-positive samples compared to NAAT-positive/CRT-negative samples (p<0.001). Human cell load did not differ between true-positive and false-negative CRT results (p = 0.835). Sensitivity of CRT in samples with low Ct load was 12.5% (95% CI, 5.2%-24.2%) and in samples with high Ct load 73.5% (95% CI, 59.9%-84.4%).
Conclusions: The sensitivity of CRT for detecting urogenital Ct in this non-manufacturer-sponsored study did not meet the expectations as described previously. The CRT missed samples with a low Ct load. Improved POC are needed as meaningful diagnostic to reduce the disease burden of Ct.
Conflict of interest statement
Figures
References
-
- World Health Organization. Global prevalence and incidence of selected curable sexually transmitted infections: Overview and estimates. Geneva, Switzerland: World Health Organization, 2001; Available: http://www.who.int/hiv/pub/sti/pub7/en/ Accessed 2012 Jan 30.
-
- Datta SD, Sternberg M, Johnson RE, Berman S, Papp JR, et al. Gonorrhea and chlamydia in the United States among persons 14 to 39 years of age, 1999 to 2002. Ann Intern Med. 2007;147:89–96. - PubMed
-
- Farley TA, Cohen DA, Elkins W. Asymptomatic sexually transmitted diseases: the case for screening. Prev Med. 2003;36:502–509. - PubMed
-
- Land JA, van Bergen JE, Morre SA, Postma MJ. Epidemiology of Chlamydia trachomatis infection in women and the cost-effectiveness of screening. Hum Reprod Update. 2010;16:189–204. - PubMed
-
- Peeling RW, Mabey D, Herring A, Hook EW. Why do we need quality-assured diagnostic tests for sexually transmitted infections? Nat Rev Microbiol. 2006;4:S7–19. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
