

Measuring and estimating GFR and treatment effect in ADPKD patients: results and implications of a longitudinal cohort study
- PMID: 22393413
- PMCID: PMC3291245
- DOI: 10.1371/journal.pone.0032533
Measuring and estimating GFR and treatment effect in ADPKD patients: results and implications of a longitudinal cohort study
Abstract
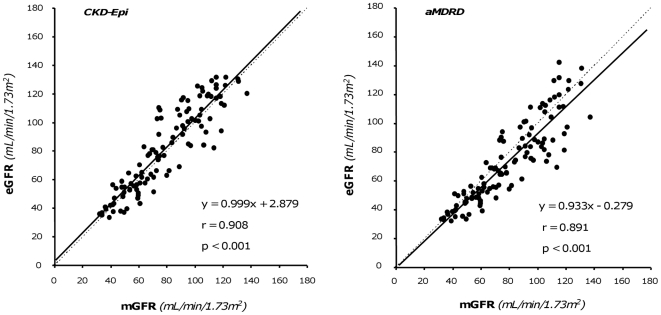
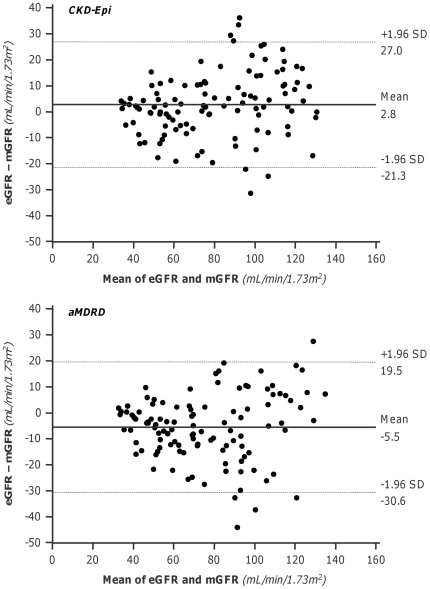
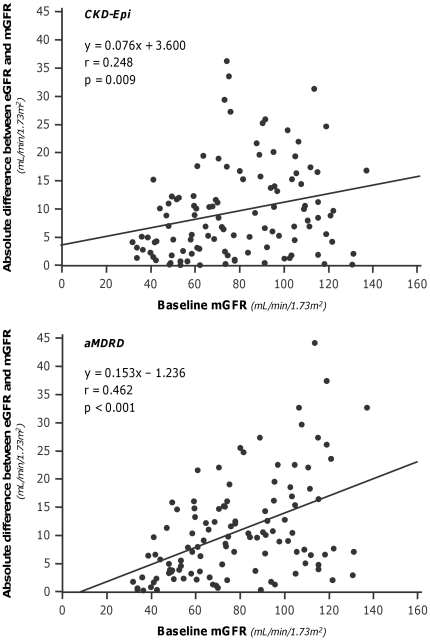
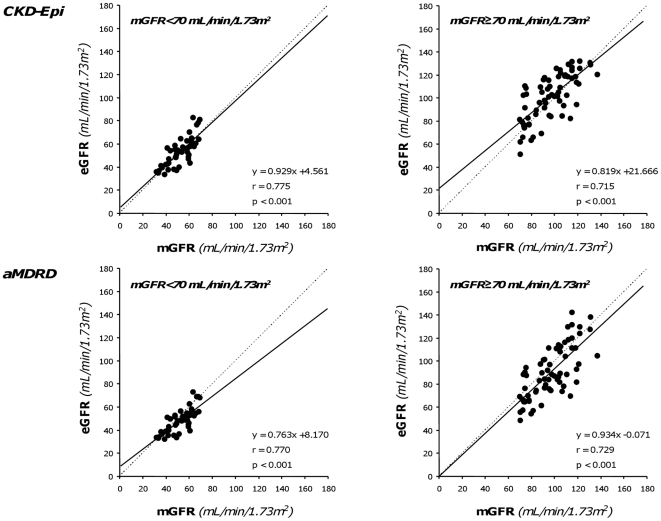
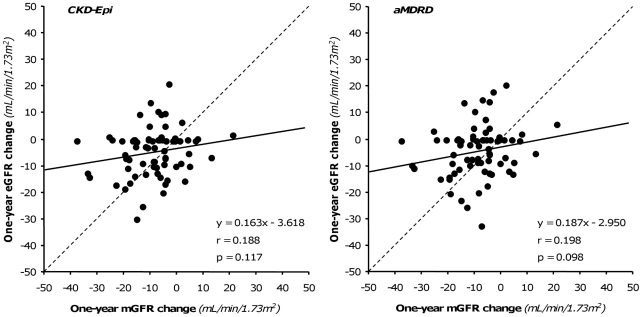
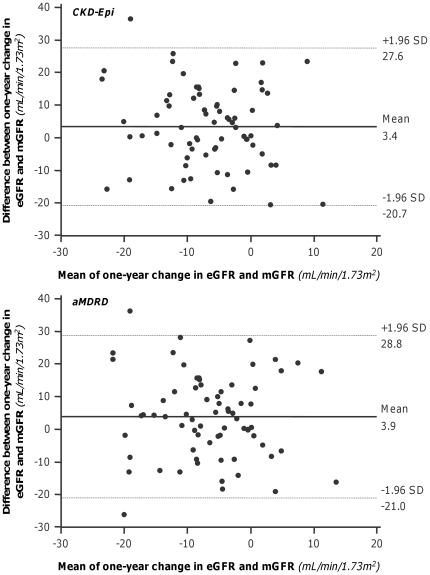
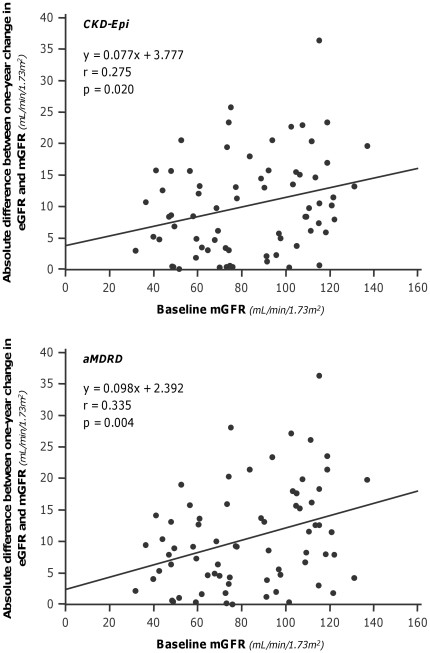
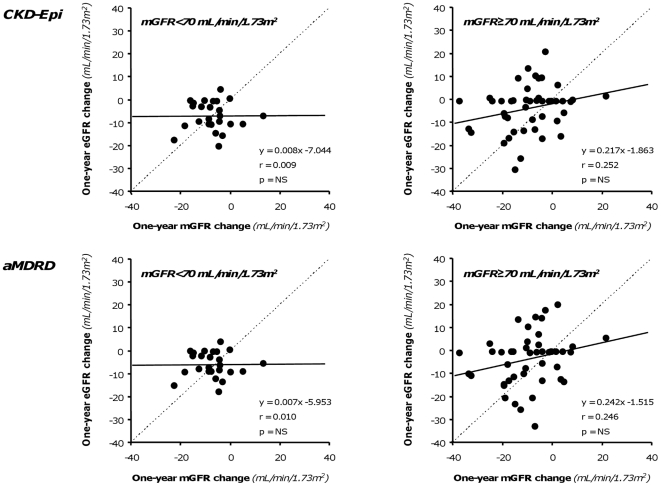
Trials failed to demonstrate protective effects of investigational treatments on glomerular filtration rate (GFR) reduction in Autosomal Dominant Polycystic Kidney Disease (ADPKD). To assess whether above findings were explained by unreliable GFR estimates, in this academic study we compared GFR values centrally measured by iohexol plasma clearance with corresponding values estimated by Chronic Kidney Disease Epidemiology Collaboration (CKD-Epi) and abbreviated Modification of Diet in Renal Disease (aMDRD) formulas in ADPKD patients retrieved from four clinical trials run by a Clinical Research Center and five Nephrology Units in Italy. Measured baseline GFRs and one-year GFR changes averaged 78.6±26.7 and 8.4±10.3 mL/min/1.73 m(2) in 111 and 71 ADPKD patients, respectively. CKD-Epi significantly overestimated and aMDRD underestimated baseline GFRs. Less than half estimates deviated by <10% from measured values. One-year estimated GFR changes did not detect measured changes. Both formulas underestimated GFR changes by 50%. Less than 9% of estimates deviated <10% from measured changes. Extent of deviations even exceeded that of measured one-year GFR changes. In ADPKD, prediction formulas unreliably estimate actual GFR values and fail to detect their changes over time. Direct kidney function measurements by appropriate techniques are needed to adequately evaluate treatment effects in clinics and research.
Conflict of interest statement
Figures
References
-
- Torres VE, Harris PC, Pirson Y. Autosomal dominant polycystic kidney disease. Lancet. 2007;369:1287–1301. - PubMed
-
- Dalgaard OZ. Bilateral polycystic disease of the kidneys; a follow-up of two hundred and eighty-four patients and their families. Acta Med Scand. 1957;Suppl 328:1–255. - PubMed
-
- Stengel B, Billon S, Van Dijk PC, Jager KJ, Dekker FW, et al. Trends in the incidence of renal replacement therapy for end-stage renal disease in Europe, 1990–1999. Nephrol Dial Transplant. 2003;18:1824–1833. - PubMed
-
- King BF, Reed JE, Bergstralh EJ, Sheedy PF, 2nd, Torres VE. Quantification and longitudinal trends of kidney, renal cyst, and renal parenchyma volumes in autosomal dominant polycystic kidney disease. J Am Soc Nephrol. 2000;11:1505–1511. - PubMed
-
- Gabow PA. Autosomal dominant polycystic kidney disease. N Engl J Med. 1993;329:332–342. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
