

Hypokinesia without decrement distinguishes progressive supranuclear palsy from Parkinson's disease
- PMID: 22396397
- PMCID: PMC3326257
- DOI: 10.1093/brain/aws038
Hypokinesia without decrement distinguishes progressive supranuclear palsy from Parkinson's disease
Abstract
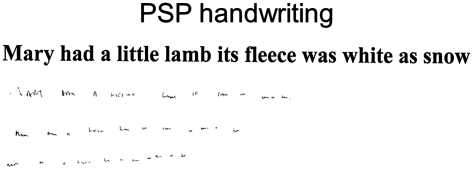
Repetitive finger tapping is commonly used to assess bradykinesia in Parkinson's disease. The Queen Square Brain Bank diagnostic criterion of Parkinson's disease defines bradykinesia as 'slowness of initiation with progressive reduction in speed and amplitude of repetitive action'. Although progressive supranuclear palsy is considered an atypical parkinsonian syndrome, it is not known whether patients with progressive supranuclear palsy have criteria-defined bradykinesia. This study objectively assessed repetitive finger tap performance and handwriting in patients with Parkinson's disease (n = 15), progressive supranuclear palsy (n = 9) and healthy age- and gender-matched controls (n = 16). The motion of the hand and digits was recorded in 3D during 15-s repetitive index finger-to-thumb tapping trials. The main finding was hypokinesia without decrement in patients with progressive supranuclear palsy, which differed from the finger tap pattern in Parkinson's disease. Average finger separation amplitude in progressive supranuclear palsy was less than half of that in controls and Parkinson's disease (P < 0.001 in both cases). Change in tap amplitude over consecutive taps was computed by linear regression. The average amplitude slope in progressive supranuclear palsy was nearly zero (0.01°/cycle) indicating a lack of decrement, which differed from the negative slope in patients with Parkinson's disease OFF levodopa (-0.20°/cycle, P = 0.002). 'Hypokinesia', defined as <50% of control group's mean amplitude, combined with 'absence of decrement', defined as mean positive amplitude slope, were identified in 87% of finger tap trials in the progressive supranuclear palsy group and only 12% in the Parkinson's disease OFF levodopa group. In progressive supranuclear palsy, the mean amplitude was not correlated with disease duration or other clinimetric scores. In Parkinson's disease, finger tap pattern was compatible with criteria-defined bradykinesia, characterized by slowness with progressive reduction in amplitude and speed and increased variability in speed throughout the tap trial. In Parkinson's disease, smaller amplitude, slower speed and greater speed variability were all associated with a more severe Unified Parkinson's Disease Rating Scale motor score. Analyses of handwriting showed that micrographia, defined as smaller than 50% of the control group's mean script size, was present in 75% of patients with progressive supranuclear palsy and 15% of patients with Parkinson's disease (P = 0.022). Most scripts performed by patients with progressive supranuclear palsy did not exhibit decrements in script size. In conclusion, patients with progressive supranuclear palsy have a specific finger tap pattern of 'hypokinesia without decrement' and they do not have criteria-defined limb bradykinesia. Similarly, 'micrographia' and 'lack of decrement in script size' are also more common in progressive supranuclear palsy than in Parkinson's disease.
Figures






References
-
- Agostino R, Berardelli A, Formica A, Stocchi F, Accornero N, Manfredi M. Analysis of repetitive and nonrepetitive sequential arm movements in patients with parkinson's disease. Mov Disord. 1994;9:311–4. - PubMed
-
- Agostino R, Berardelli A, Curra A, Accornero N, Manfredi M. Clinical impairment of sequential finger movements in parkinson's disease. Mov Disord. 1998;13:418–21. - PubMed
-
- Agostino R, Curra A, Giovannelli M, Modugno N, Manfredi M, Berardelli A. Impairment of individual finger movements in parkinson's disease. Mov Disord. 2003;18:560–5. - PubMed
-
- Alexander GE, Crutcher MD. Functional architecture of basal ganglia circuits: Neural substrates of parallel processing. Trends Neurosci. 1990;13:266–71. - PubMed
-
- Bajaj NP, Gontu V, Birchall J, Patterson J, Grosset DG, Lees AJ. Accuracy of clinical diagnosis in tremulous parkinsonian patients: a blinded video study. J Neurol Neurosurg Psychiatry. 2010;81:1223–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
