

Ischemic preconditioning in the younger and aged heart
- PMID: 22396871
- PMCID: PMC3295052
Ischemic preconditioning in the younger and aged heart
Abstract
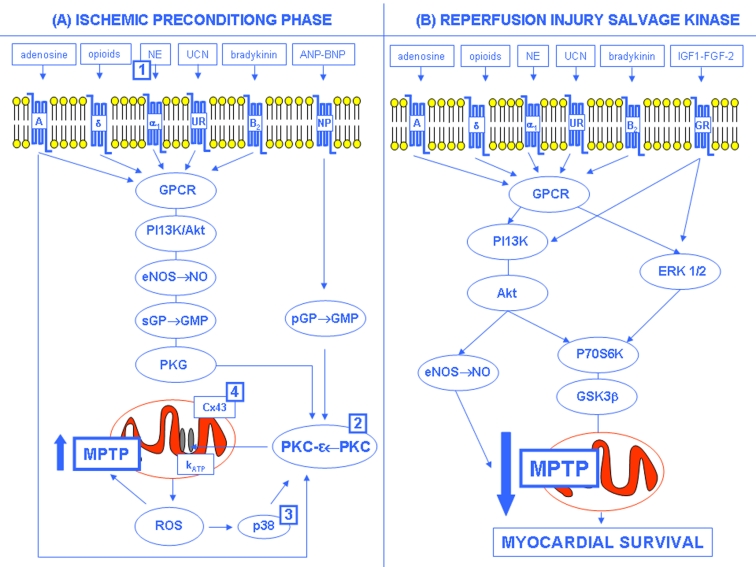
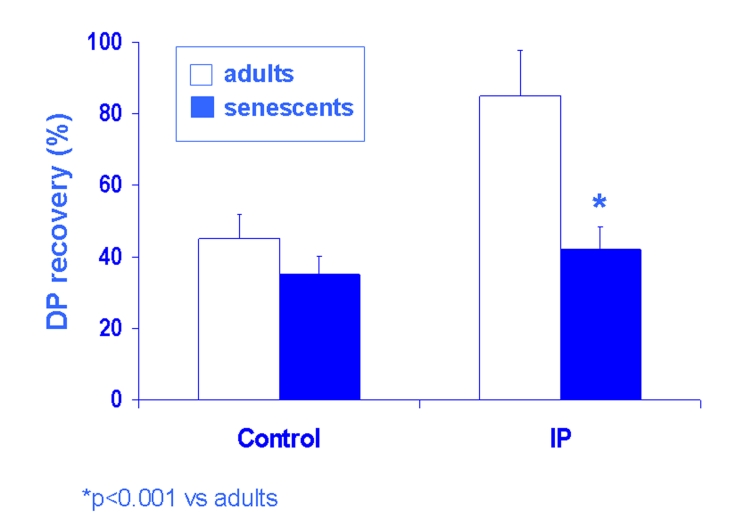
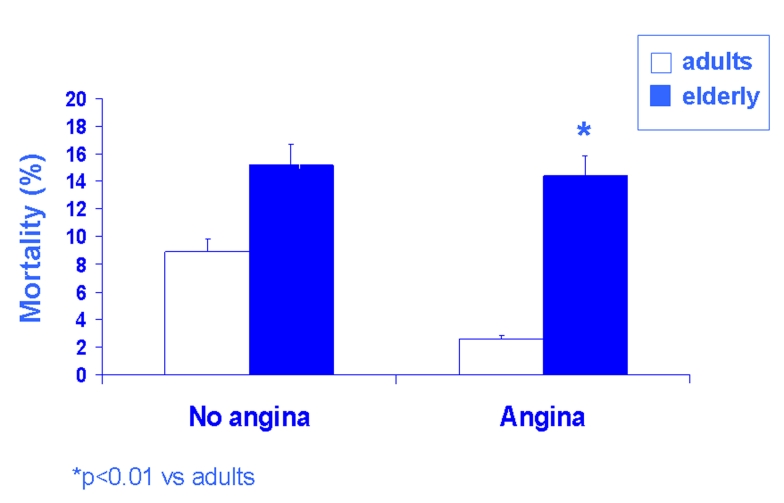
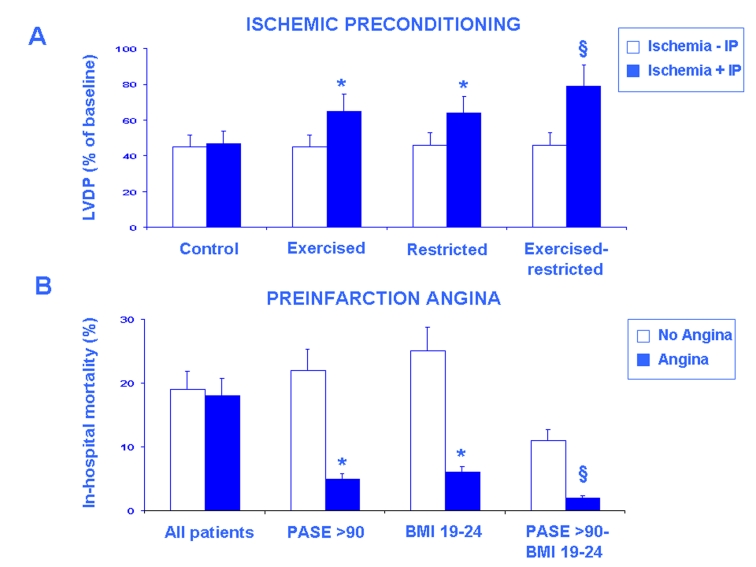
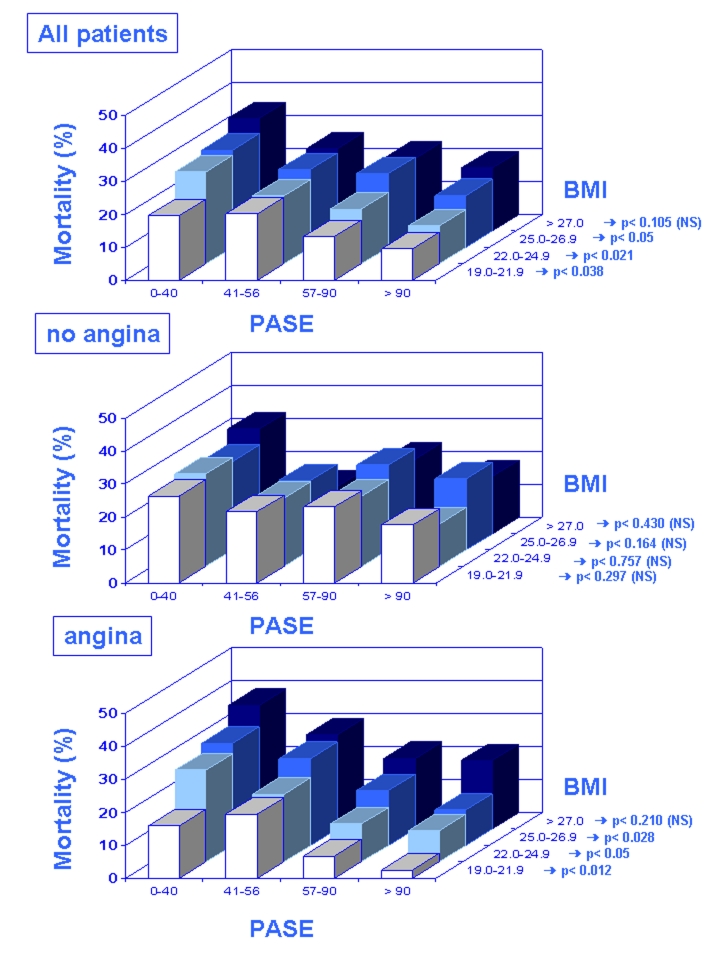
Ischemic preconditioning is the effect of brief ischemic episodes which protect the heart from the following more prolonged ischemic episode. This mechanism is effective in younger but not in aged heart. The age-related reduction of ischemic preconditioning has been demonstrated in experimental models and in elderly patients. Preinfarction angina, a clinical equivalent of ischemic preconditioning, reduces mortality in adult but not in elderly patients with acute myocardial infarction. Physical activity or caloric restriction is partially capable to preserve the cardioprotective effect of ischemic preconditioning in the aging heart. More importantly, physical activity and caloric restriction in tandem action completely preserve the protective mechanism of ischemic preconditioning. Accordingly, the protective mechanism of preinfarction angina is preserved in elderly patients with a high grade of physical activity or a low body-mass index. Thus, both physical activity and caloric restriction are confirmed as powerful anti-aging interventions capable to restore age-dependent reduction of a critical endogenous protective mechanism such as ischemic preconditioning.
Keywords: Aged; caloric restriction; heart; ischemia; preconditioning; younger.
Figures
References
-
- Murry CE, Jennings RB, Reimer KA. Preconditioning with ischemia: a delay of lethal cell injury in ischemic myocardium. Circulation. 1986;74:1124–36. - PubMed
-
- Kloner RA, Bolli R, Marban E, Reinlib L, Braunwald E. Medical and cellular implications of stunning, hibernation and preconditioning. An NHLBI workshop. Circulation. 1998;97:1848–67. - PubMed
-
- Napoli C, Pinto A, Cirino G. Pharmacological modulation, preclinical studies, and new clinical features of myocardial ischemic preconditioning. Pharmacol Ther. 2000;88:311–31. - PubMed
-
- Yellon DM, Downey JM. Preconditioning the myocardium: from cellular physiology to clinical cardiology. Physiol Rev. 2003;83:1113–51. - PubMed
-
- Vinten-Johansen J, Zhao ZQ, Jiang R, Zatta AJ, Dobson GP. Preconditioning and postconditioning: innate cardioprotection from ischemia-reperfusion injury. J Appl Physiol. 2007;103:1441–8. - PubMed
LinkOut - more resources
Full Text Sources