

Total pancreatectomy and islet autotransplantation for chronic pancreatitis
- PMID: 22397977
- PMCID: PMC3755128
- DOI: 10.1016/j.jamcollsurg.2011.12.040
Total pancreatectomy and islet autotransplantation for chronic pancreatitis
Abstract
Background: Total pancreatectomy (TP) with intraportal islet autotransplantation (IAT) can relieve pain and preserve β-cell mass in patients with chronic pancreatitis (CP) when other therapies fail. We report on a >30-year single-center series.
Study design: Four hundred and nine patients (including 53 children, 5 to 18 years) with CP underwent TP-IAT from February 1977 to September 2011 (etiology: idiopathic, 41%; Sphincter of Oddi dysfunction/biliary, 9%; genetic, 14%; divisum, 17%; alcohol, 7%; and other, 12%; mean age was 35.3 years, 74% were female; 21% has earlier operations, including 9% Puestow procedure, 6% Whipple, 7% distal pancreatectomy, and 2% other). Islet function was classified as insulin independent for those on no insulin; partial, if known C-peptide positive or euglycemic on once-daily insulin; and insulin dependent if on standard basal-bolus diabetic regimen. A 36-item Short Form (SF-36) survey for quality of life was completed by patients before and in serial follow-up since 2007, with an integrated survey that was added in 2008.
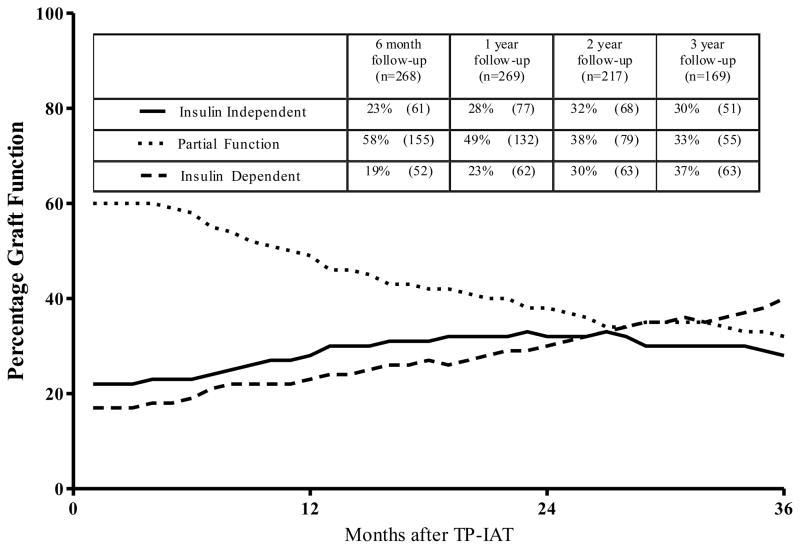
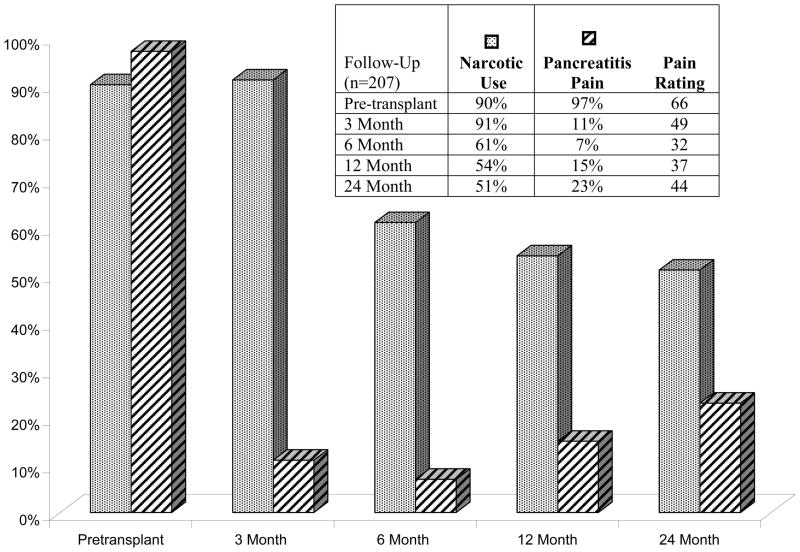
Results: Actuarial patient survival post TP-IAT was 96% in adults and 98% in children (1 year) and 89% and 98% (5 years). Complications requiring relaparotomy occurred in 15.9% and bleeding (9.5%) was the most common complication. IAT function was achieved in 90% (C-peptide >0.6 ng/mL). At 3 years, 30% were insulin independent (25% in adults, 55% in children) and 33% had partial function. Mean hemoglobin A1c was <7.0% in 82%. Earlier pancreas surgery lowered islet yield (2,712 vs 4,077/kg; p = 0.003). Islet yield (<2,500/kg [36%]; 2,501 to 5,000/kg [39%]; >5,000/kg [24%]) correlated with degree of function with insulin-independent rates at 3 years of 12%, 22%, and 72%, and rates of partial function 33%, 62%, and 24%. All patients had pain before TP-IAT and nearly all were on daily narcotics. After TP-IAT, 85% had pain improvement. By 2 years, 59% had ceased narcotics. All children were on narcotics before, 39% at follow-up; pain improved in 94%; and 67% became pain-free. In the SF-36 survey, there was significant improvement from baseline in all dimensions, including the Physical and Mental Component Summaries (p < 0.01), whether on narcotics or not.
Conclusions: TP can ameliorate pain and improve quality of life in otherwise refractory CP patients, even if narcotic withdrawal is delayed or incomplete because of earlier long-term use. IAT preserves meaningful islet function in most patients and substantial islet function in more than two thirds of patients, with insulin independence occurring in one quarter of adults and half the children.
Copyright © 2012 American College of Surgeons. Published by Elsevier Inc. All rights reserved.
Figures



References
-
- Braganza J, Lee S, McCloy R, McMahon M. Chronic pancreatitis. Lancet. 2011;377(9772):1184–1197. - PubMed
-
- Ahmad S, Wray C, Rilo H, et al. Chronic pancreatitis: recent advances and ongoing challenges. Curr Probl Surg. 2006;43:127–238. - PubMed
-
- Andersen DK, Frey CF. The Evolution of the surgical treatment of chronic pancreatitis. Ann Surg. 2010;251:18–32. - PubMed
-
- Khanna S, Tandon RK. Endotherapy for pain in chronic pancreatitis. J of Gastroenterology and Hepatology. 2008;23:1649–1656. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
