

Utility of serum procalcitonin values in patients with acute exacerbations of chronic obstructive pulmonary disease: a cautionary note
- PMID: 22399852
- PMCID: PMC3292390
- DOI: 10.2147/COPD.S29149
Utility of serum procalcitonin values in patients with acute exacerbations of chronic obstructive pulmonary disease: a cautionary note
Abstract
Background: Serum procalcitonin levels have been used as a biomarker of invasive bacterial infection and recently have been advocated to guide antibiotic therapy in patients with chronic obstructive pulmonary disease (COPD). However, rigorous studies correlating procalcitonin levels with microbiologic data are lacking. Acute exacerbations of COPD (AECOPD) have been linked to viral and bacterial infection as well as noninfectious causes. Therefore, we evaluated procalcitonin as a predictor of viral versus bacterial infection in patients hospitalized with AECOPD with and without evidence of pneumonia.
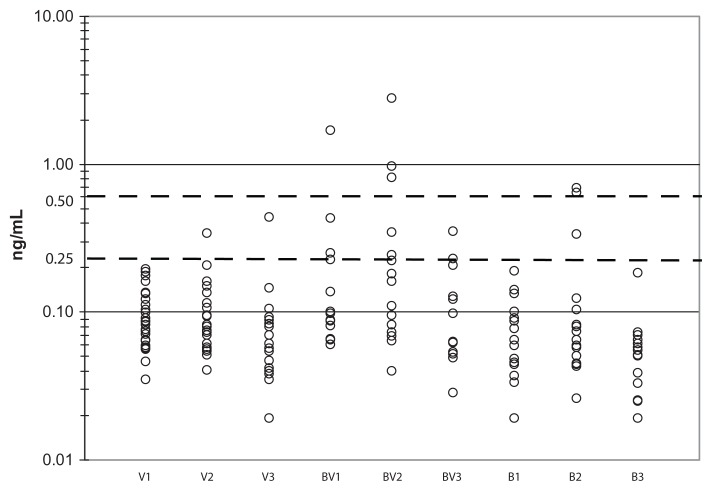
Methods: Adults hospitalized during the winter with symptoms consistent with AECOPD underwent extensive testing for viral, bacterial, and atypical pathogens. Serum procalcitonin levels were measured on day 1 (admission), day 2, and at one month. Clinical and laboratory features of subjects with viral and bacterial diagnoses were compared.
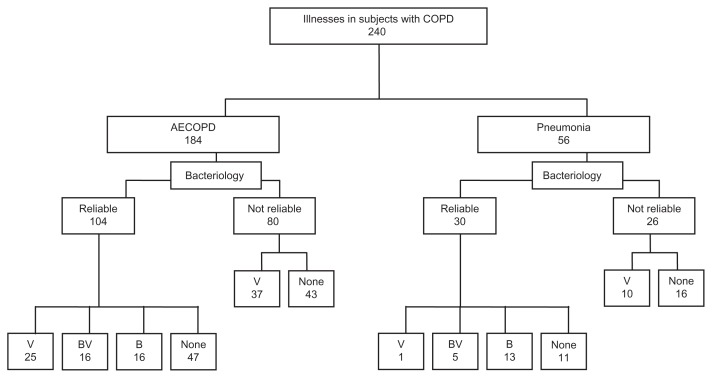
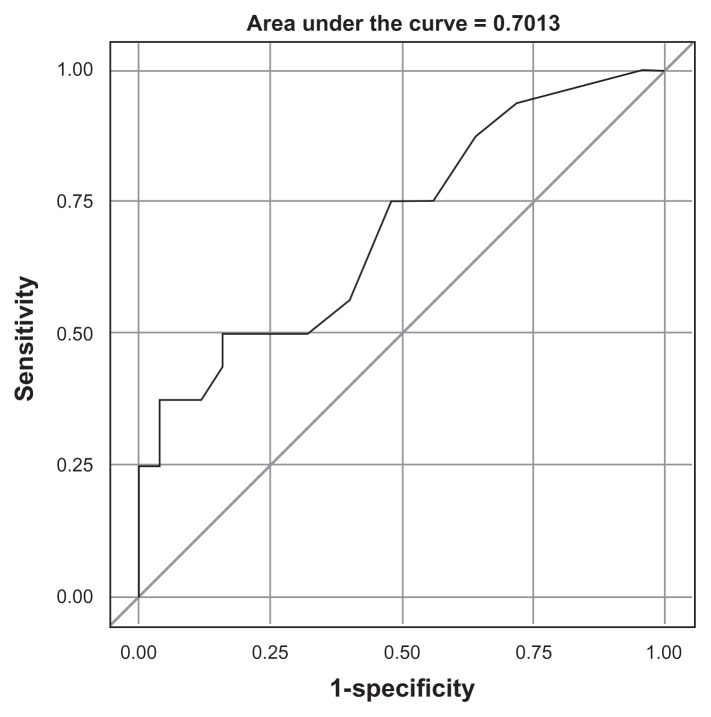
Results: In total, 224 subjects with COPD were admitted for 240 respiratory illnesses. Of these, 56 had pneumonia and 184 had AECOPD alone. A microbiologic diagnosis was made in 76 (56%) of 134 illnesses with reliable bacteriology (26 viral infection, 29 bacterial infection, and 21 mixed viral bacterial infection). Mean procalcitonin levels were significantly higher in patients with pneumonia compared with AECOPD. However, discrimination between viral and bacterial infection using a 0.25 ng/mL threshold for bacterial infection in patients with AECOPD was poor.
Conclusion: Procalcitonin is useful in COPD patients for alerting clinicians to invasive bacterial infections such as pneumonia but it does not distinguish bacterial from viral and noninfectious causes of AECOPD.
Keywords: bacterial infection; bronchitis; chronic obstructive pulmonary disease; procalcitonin; virus.
Figures
References
-
- Pauwels RA, Buist AS, Calverley PM, Jenkins CR, Hurd SS GOLD Scientific Committee. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO global initiative for chronic obstructive lung disease (GOLD) workshop summary. Am J Respir Crit Care Med. 2001;163(5):1256–1276. - PubMed
-
- Ram FS, Rodriguez-Roisin R, Granados-Navarrete A, Garcia-Aymerich J, Barnes NC. Antibiotics for exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2006;2:CD004403. - PubMed
-
- Monso E, Ruiz J, Rosell A, et al. Bacterial infection in chronic obstructive pulmonary disease. A study of stable and exacerbated outpatients using the protected specimen brush. Am J Respir Crit Care Med. 1995;152(4 Pt 1):1316–1320. - PubMed
-
- Kherad O, Rutschmann OT. Viral infections as a cause of chronic obstructive pulmonary disease (COPD) exacerbation. Praxis (Bern 1994) 2010;99(4):235–240. German. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
