

Primary care provider perceptions of the effectiveness of two self-management support programs for vulnerable patients with diabetes
- PMID: 22401329
- PMCID: PMC3320828
- DOI: 10.1177/193229681200600114
Primary care provider perceptions of the effectiveness of two self-management support programs for vulnerable patients with diabetes
Abstract
Background: Primary care providers (PCPs) in safety net settings face barriers to optimizing care for patients with diabetes. We conducted this study to assess PCPs' perspectives on the effectiveness of two language-concordant diabetes self-management support programs.
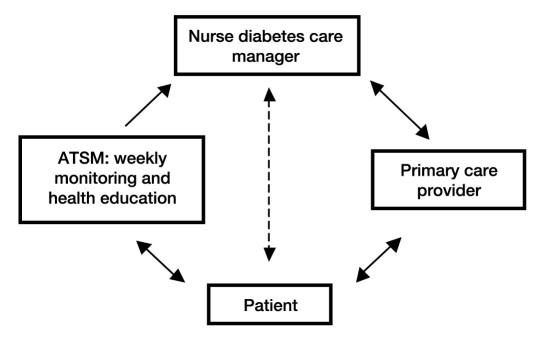
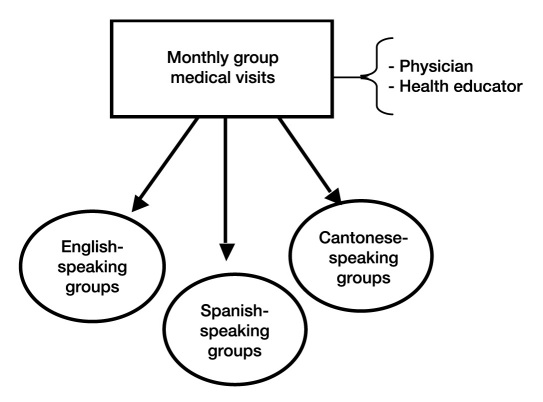
Methods: One year postintervention, we surveyed PCPs whose patients with diabetes participated in a three-arm multiclinic randomized controlled trial comparing usual care (UC), weekly automated telephone self-management (ATSM) support with nurse care management, and monthly group medical visits (GMVs). We compared PCP perspectives on patient activation to create and achieve goals, quality of care, and barriers to care using regression models accounting for within-PCP clustering.
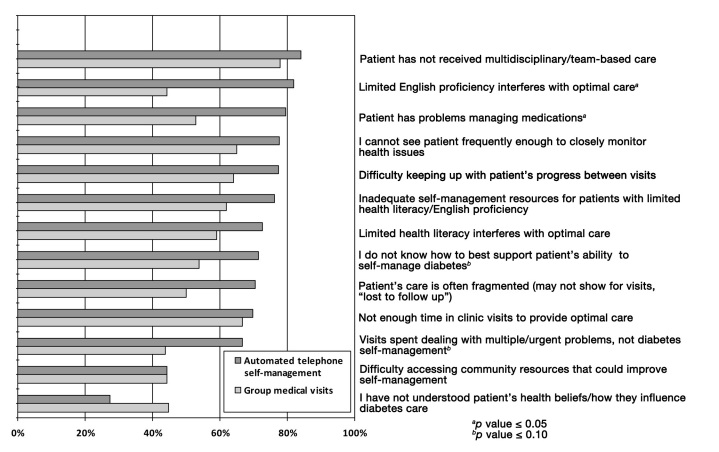
Results: Of 113 eligible PCPs caring for 330 enrolled patients, 87 PCPs (77%) responded to surveys about 245 (74%) enrolled patients. Intervention patients were more likely to be perceived by PCPs as activated to create and achieve goals for chronic care when compared with UC patients (standardized effect size, ATSM vs UC, +0.41, p = 0.01; GMV vs UC, +0.31, p = 0.05). Primary care providers rated quality of care as higher for patients exposed to ATSM compared to UC (odds ratio 3.6, p < 0.01). Compared with GMV patients, ATSM patients were more likely to be perceived by PCPs as overcoming barriers related to limited English proficiency (82% ATSM vs 44% GMV, p = 0.01) and managing medications (80% ATSM vs 53% GMV, p = 0.01).
Conclusions: Primary care providers perceived that patients receiving ATSM support had overcome barriers, participated more actively, and received higher quality diabetes care. These views of clinician stakeholders lend additional evidence for the potential to upscale ATSM more broadly to support PCPs in their care of diverse, multilinguistic populations.
© 2012 Diabetes Technology Society.
Figures
Similar articles
-
Effects of self-management support on structure, process, and outcomes among vulnerable patients with diabetes: a three-arm practical clinical trial.Diabetes Care. 2009 Apr;32(4):559-66. doi: 10.2337/dc08-0787. Epub 2009 Jan 8. Diabetes Care. 2009. PMID: 19131469 Free PMC article. Clinical Trial.
-
Quasi-experimental trial of diabetes Self-Management Automated and Real-Time Telephonic Support (SMARTSteps) in a Medicaid managed care plan: study protocol.BMC Health Serv Res. 2012 Jan 26;12:22. doi: 10.1186/1472-6963-12-22. BMC Health Serv Res. 2012. PMID: 22280514 Free PMC article. Clinical Trial.
-
Cost-effectiveness of automated telephone self-management support with nurse care management among patients with diabetes.Ann Fam Med. 2008 Nov-Dec;6(6):512-8. doi: 10.1370/afm.889. Ann Fam Med. 2008. PMID: 19001303 Free PMC article. Clinical Trial.
-
Closing the gap: eliminating health care disparities among Latinos with diabetes using health information technology tools and patient navigators.J Diabetes Sci Technol. 2012 Jan 1;6(1):169-76. doi: 10.1177/193229681200600121. J Diabetes Sci Technol. 2012. PMID: 22401336 Free PMC article. Review.
-
Telemedicine in Complex Diabetes Management.Curr Diab Rep. 2018 May 24;18(7):42. doi: 10.1007/s11892-018-1015-3. Curr Diab Rep. 2018. PMID: 29797292 Review.
Cited by
-
Effectiveness of Telemedicine in Controlling Hyperglycemia Among Diabetic Patients on Insulin Therapy in Primary Care: A Systematic Review and Meta-Analysis.Cureus. 2023 Dec 6;15(12):e50045. doi: 10.7759/cureus.50045. eCollection 2023 Dec. Cureus. 2023. PMID: 38077677 Free PMC article. Review.
-
Using Patient-Generated Health Data From Mobile Technologies for Diabetes Self-Management Support: Provider Perspectives From an Academic Medical Center.J Diabetes Sci Technol. 2014 Jan;8(1):74-82. doi: 10.1177/1932296813511727. Epub 2014 Jan 1. J Diabetes Sci Technol. 2014. PMID: 24876541 Free PMC article.
-
Automated telephone communication systems for preventive healthcare and management of long-term conditions.Cochrane Database Syst Rev. 2016 Dec 14;12(12):CD009921. doi: 10.1002/14651858.CD009921.pub2. Cochrane Database Syst Rev. 2016. PMID: 27960229 Free PMC article.
-
Sex and Race/Ethnicity Differences in Following Dietary and Exercise Recommendations for U.S. Representative Sample of Adults With Type 2 Diabetes.Am J Mens Health. 2017 Mar;11(2):380-391. doi: 10.1177/1557988316681126. Epub 2016 Dec 7. Am J Mens Health. 2017. PMID: 27932589 Free PMC article.
-
Health care professionals' views towards self-management and self-management education for people with type 2 diabetes.BMJ Open. 2019 Jul 16;9(7):e029961. doi: 10.1136/bmjopen-2019-029961. BMJ Open. 2019. PMID: 31315874 Free PMC article.
References
-
- Varkey AB, Manwell LB, Williams ES, Ibrahim SA, Brown RL, Bobula JA, Horner-Ibler BA, Schwartz MD, Konrad TR, Wiltshire JC, Linzer M MEMO Investigators. Separate and unequal: clinics where minority and nonminority patients receive primary care. Arch Intern Med. 2009;169(3):243–250. - PubMed
-
- Linzer M, Manwell LB, Williams ES, Bobula JA, Brown RL, Varkey AB, Man B, McMurray JE, Maguire A, Horner-Ibler B, Schwartz MD MEMO (Minimizing Error, Maximizing Outcome) Investigators. Working conditions in primary care: physician reactions and care quality. Ann Intern Med. 2009;151(1):28–36. W6-9. - PubMed
-
- Lewin ME, Altman SH Institute of Medicine. America's Health Care Safety Net. Washington, D.C: National Academy Press; 2000. Committee on the Changing Market, Managed Care, and the Future Viability of Safety Net Providers; p. 281.
-
- Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, D.C: National Academy Press; 2001. Committee on Quality of Health Care in America.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
