

Factors predisposing to claims and compensations for patient injuries following total hip and knee arthroplasty
- PMID: 22401679
- PMCID: PMC3339536
- DOI: 10.3109/17453674.2012.672089
Factors predisposing to claims and compensations for patient injuries following total hip and knee arthroplasty
Abstract
Background and purpose: Factors associated with malpractice claims are poorly understood. Knowledge of these factors could help to improve patient safety. We investigated whether patient characteristics and hospital volume affect claims and compensations following total hip arthroplasty (THA) and knee arthroplasty (TKA) in a no-fault scheme.
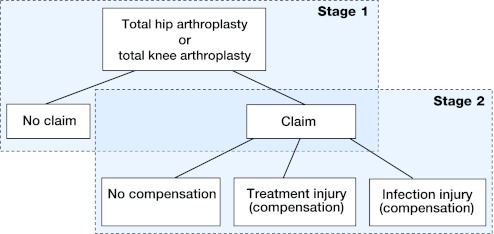
Methods: A retrospective registry-based study was done on 16,646 THAs and 17,535 TKAs performed in Finland from 1998 through 2003. First, the association between patient characteristics-e.g., age, sex, comorbidity, prosthesis type-and annual hospital volume with filing of a claim was analyzed by logistic regression. Then, multinomial logistic regression was applied to analyze the association between these same factors and receipt of compensation.
Results: For THA and TKA, patients over 65 years of age were less likely to file a claim than patients under 65 (OR = 0.57, 95% CI: 0.46-0.72 and OR = 0.65, CI: 0.53-0.80, respectively), while patients with increased comorbidity were more likely to file a claim (OR = 1.17, CI: 1.04-1.31 and OR = 1.14, CI: 1.03-1.26, respectively). Following THA, male sex and cemented prosthesis reduced the odds of a claim (OR = 0.74, CI: 0.60-0.91 and OR = 0.77, CI: 0.60-0.99, respectively) and volume of between 200 and 300 operations increased the odds of a claim (OR = 1.29, CI: 1.01-1.64). Following TKA, a volume of over 300 operations reduced the probability of compensation for certain injury types (RRR = 0.24, CI: 0.08-0.72).
Interpretation: Centralization of TKA to hospitals with higher volume may reduce the rate of compensable patient injuries. Furthermore, more attention should be paid to equal opportunities for patients to file a claim and obtain compensation.
Figures
Comment in
-
Patient injuries in primary total hip replacement.Acta Orthop. 2016 Jun;87(3):209-17. doi: 10.3109/17453674.2015.1135662. Epub 2016 Jan 25. Acta Orthop. 2016. PMID: 26808350 Free PMC article.
References
-
- Ahmad R, Sharma V, Sandhu H, Bishay M. Leg length discrepancy in total hip arthroplasty with the use of cemented and uncemented femoral stems. A prospective radiological study. Hip Int. 2009;19(3):264–7. - PubMed
-
- Battaglia TC, Mulhall KJ, Brown TE, Saleh KJ. Increased surgical volume is associated with lower THA dislocation rates. Clin Orthop. 2006;(447):28–33. - PubMed
-
- Berry DJ. Epidemiology: Hip and knee. Orthop Clin North Am. 1999;30(2):183–90. - PubMed
-
- Bismark MM, Brennan TA, Davis PB, Studdert DM. Claiming behaviour in a no-fault system of medical injury: A descriptive analysis of claimants and non-claimants. Med J Aust. 2006;185(4):203–7. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical