

High STOP-Bang score indicates a high probability of obstructive sleep apnoea
- PMID: 22401881
- PMCID: PMC3325050
- DOI: 10.1093/bja/aes022
High STOP-Bang score indicates a high probability of obstructive sleep apnoea
Abstract
Background: The STOP-Bang questionnaire is used to screen patients for obstructive sleep apnoea (OSA). We evaluated the association between STOP-Bang scores and the probability of OSA.
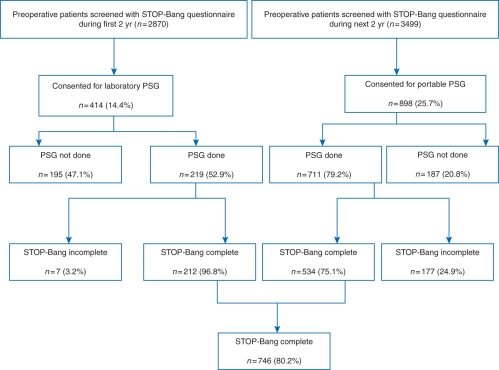
Methods: After Institutional Review Board approval, patients who visited the preoperative clinics for a scheduled inpatient surgery were approached for informed consent. Patients answered STOP questionnaire and underwent either laboratory or portable polysomnography (PSG). PSG recordings were scored manually. The BMI, age, neck circumference, and gender (Bang) were documented. Over 4 yr, 6369 patients were approached and 1312 (20.6%) consented. Of them, 930 completed PSG, and 746 patients with complete data on PSG and STOP-Bang questionnaire were included for data analysis.
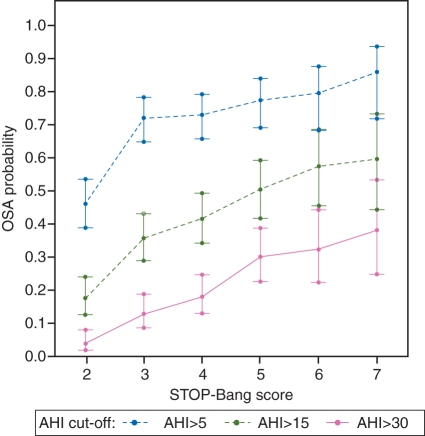
Results: The median age of 746 patients was 60 yr, 49% males, BMI 30 kg m(-2), and neck circumference 39 cm. OSA was present in 68.4% with 29.9% mild, 20.5% moderate, and 18.0% severe OSA. For a STOP-Bang score of 5, the odds ratio (OR) for moderate/severe and severe OSA was 4.8 and 10.4, respectively. For STOP-Bang 6, the OR for moderate/severe and severe OSA was 6.3 and 11.6, respectively. For STOP-Bang 7 and 8, the OR for moderate/severe and severe OSA was 6.9 and 14.9, respectively. The predicted probabilities for moderate/severe OSA increased from 0.36 to 0.60 as the STOP-Bang score increased from 3 to 7 and 8.
Conclusions: In the surgical population, a STOP-Bang score of 5-8 identified patients with high probability of moderate/severe OSA. The STOP-Bang score can help the healthcare team to stratify patients for unrecognized OSA, practice perioperative precautions, or triage patients for diagnosis and treatment.
Figures

Comment in
-
Cat of the month. STOP-Bang Questionnaire is useful for obstructive sleep apnea screening. UT CAT # 2344.Tex Dent J. 2014 Jun;131(6):420. Tex Dent J. 2014. PMID: 25163214 No abstract available.
References
-
- Young T, Hutton R, Finn L, Badr S, Palta M. The gender bias in sleep apnea diagnosis: are women missed because they have different symptoms? Arch Intern Med. 1996;156:2445–51. doi:10.1001/archinte.1996.00440200055007. - DOI - PubMed
-
- Lettieri CJ, Eliasson AH, Andrada T, Khramtsov A, Raphaelson M, Kristo DA. Obstructive sleep apnea syndrome: are we missing an at-risk population? J Clin Sleep Med. 2005;1:381–5. - PubMed
-
- Kaw R, Michota F, Jaffer A, Ghamande S, Auckley D, Golish J. Unrecognized sleep apnea in the surgical patient: implications for the perioperative setting. Chest. 2006;129:198–205. doi:10.1378/chest.129.1.198. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
