

Clinical evaluation of safety and immunogenicity of PADRE-cytomegalovirus (CMV) and tetanus-CMV fusion peptide vaccines with or without PF03512676 adjuvant
- PMID: 22402037
- PMCID: PMC3308906
- DOI: 10.1093/infdis/jis107
Clinical evaluation of safety and immunogenicity of PADRE-cytomegalovirus (CMV) and tetanus-CMV fusion peptide vaccines with or without PF03512676 adjuvant
Erratum in
- J Infect Dis. 2013 Sep;208(6):1038. Dadwal, Sanjeet [added]
Abstract
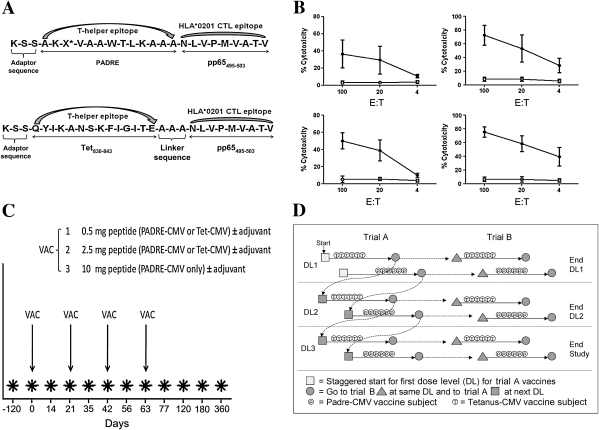
Background: It has been reported that cytomegalovirus (CMV) pp65-specific T cells can protect hematopoietic cell transplant (HCT) recipients from CMV complications. Two candidate CMV peptide vaccines composed of the HLA A*0201 pp65(495-503) cytotoxic CD8(+) T-cell epitope fused to 2 different universal T-helper epitopes (either the synthetic Pan DR epitope [PADRE] or a natural Tetanus sequence) were clinically evaluated for safety and ability to elicit pp65 T cells in HLA A*0201 healthy volunteers.
Methods: Escalating doses (0.5, 2.5, 10 mg) of PADRE or Tetanus pp65(495-503) vaccines with (30 adults) or without (28 adults) PF03512676 adjuvant were administered by subcutaneous injection every 3 weeks for a total of 4 injections.
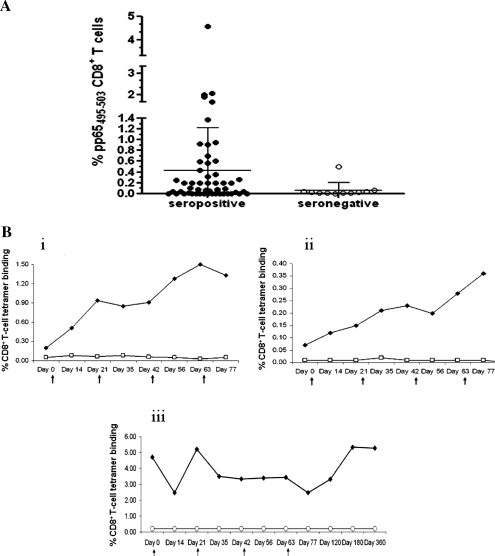
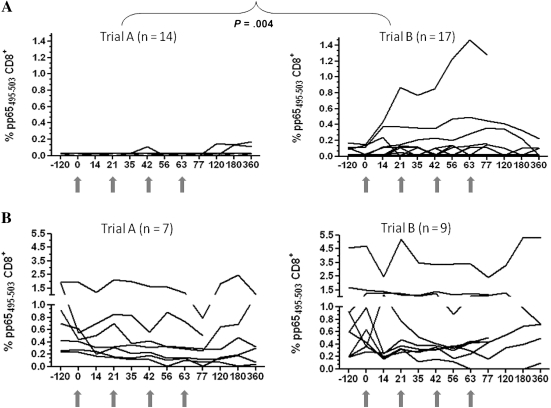
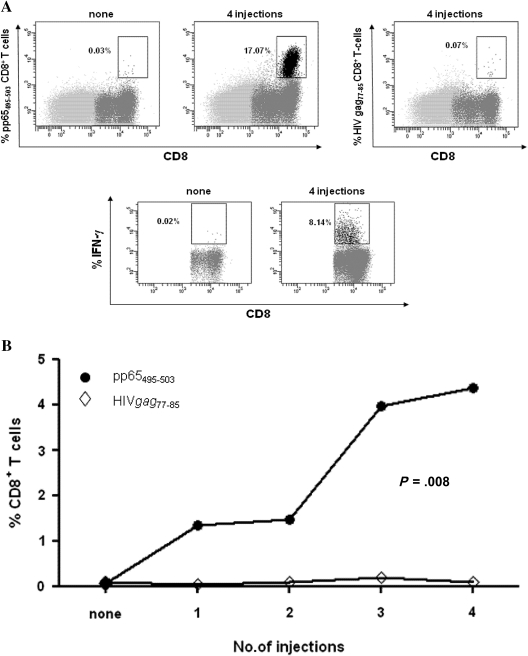
Results: No serious adverse events were reported, although vaccines used in combination with PF03512676 had enhanced reactogenicity. Ex vivo responses were detected by flow cytometry exclusively in volunteers who received the vaccine coadministered with PF03512676. In addition, using a sensitive in vitro stimulation system, vaccine-elicited pp65(495-503) T cells were expanded in 30% of volunteers injected solely with the CMV peptides and in all tested subjects receiving the vaccines coinjected with PF03512676.
Conclusions: Acceptable safety profiles and vaccine-driven expansion of pp65(495-503) T cells in healthy adults support further evaluation of CMV peptide vaccines combined with PF03512676 in the HCT setting.
Clinical trials registration: NCT00722839.
Figures
References
-
- Aubert G, Hassan-Walker AF, Madrigal JA, et al. Cytomegalovirus-specific cellular immune responses and viremia in recipients of allogeneic stem cell transplants. J Infect Dis. 2001;184:955–63. - PubMed
-
- Hakki M, Riddell SR, Storek J, et al. Immune reconstitution to cytomegalovirus after allogeneic hematopoietic stem cell transplantation: impact of host factors, drug therapy, and subclinical reactivation. Blood. 2003;102:3060–7. - PubMed
-
- Khanna R, Diamond DJ. Human cytomegalovirus vaccine: time to look for alternative options. Trends Mol Med. 2006;12:26–33. - PubMed
-
- Einsele H, Hebart H. CMV-specific immunotherapy. Hum Immunol. 2004;65:558–64. - PubMed
-
- Gamadia LE, Remmerswaal EB, Weel JF, Bemelman F, van Lier RA, ten Berge IJ. Primary immune responses to human CMV: a critical role for IFN-gamma-producing CD4+ T cells in protection against CMV disease. Blood. 2003;101:2686–92. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
