

Impact of noncardiac comorbidities on morbidity and mortality in a predominantly male population with heart failure and preserved versus reduced ejection fraction
- PMID: 22402071
- PMCID: PMC4687406
- DOI: 10.1016/j.jacc.2011.11.040
Impact of noncardiac comorbidities on morbidity and mortality in a predominantly male population with heart failure and preserved versus reduced ejection fraction
Abstract
Objectives: The aim of this study was to evaluate the prevalence and prognostic impacts of noncardiac comorbidities in patients with heart failure (HF) with preserved ejection fraction (HFpEF) compared with those with HF with reduced ejection fraction (HFrEF).
Background: There is a paucity of information on the comparative prognostic significance of comorbidities between patients with HFpEF and those with HFrEF.
Methods: In a national ambulatory cohort of veterans with HF, the comorbidity burden of 15 noncardiac comorbidities and the impacts of these comorbidities on hospitalization and mortality were compared between patients with HFpEF and those with HFrEF.
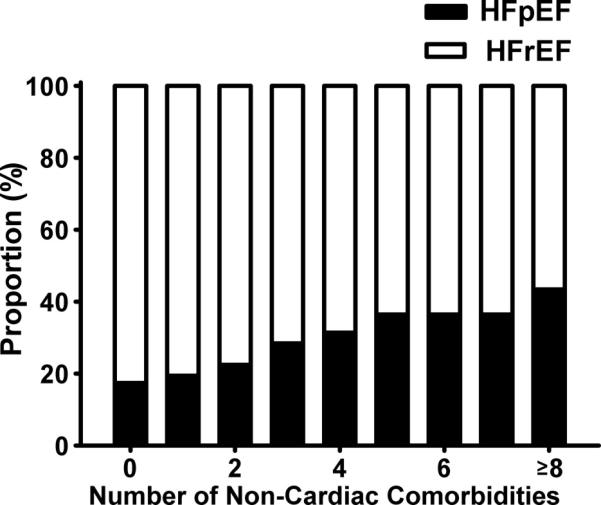
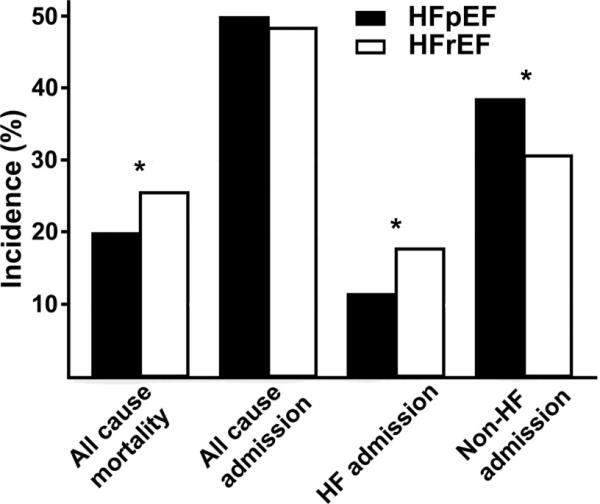
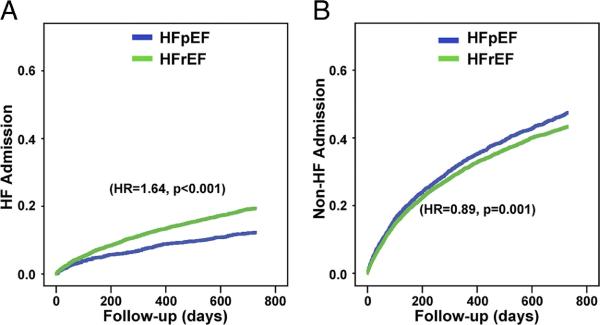
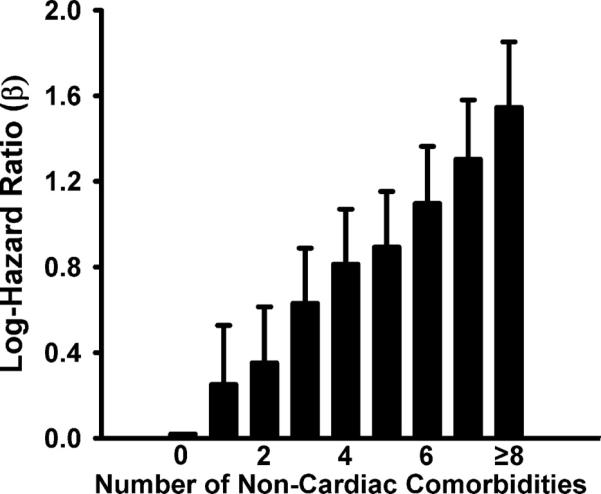
Results: The cohort consisted of 2,843 patients with HFpEF and 6,599 with HFrEF with 2-year follow-up. Compared with patients with HFrEF, those with HFpEF were older and had higher prevalence of chronic obstructive pulmonary disease, diabetes, hypertension, psychiatric disorders, anemia, obesity, peptic ulcer disease, and cancer but a lower prevalence of chronic kidney disease. Patients with HFpEF had lower HF hospitalization, higher non-HF hospitalization, and similar overall hospitalization compared with those with HFrEF (p < 0.001, p < 0.001, and p = 0.19, respectively). An Increasing number of noncardiac comorbidities was associated with a higher risk for all-cause admissions (p < 0.001). Comorbidities had similar impacts on mortality in patients with HFpEF compared with those with HFrEF, except for chronic obstructive pulmonary disease, which was associated with a higher hazard (1.62 [95% confidence interval: 1.36 to 1.92] vs. 1.23 [95% confidence interval: 1.11 to 1.37], respectively, p = 0.01 for interaction) in patients with HFpEF.
Conclusions: There is a higher noncardiac comorbidity burden associated with higher non-HF hospitalizations in patients with HFpEF compared with those with HFrEF. However, individually, most comorbidities have similar impacts on mortality in both groups. Aggressive management of comorbidities may have an overall greater prognostic impact in HFpEF compared to HFrEF.
Copyright © 2012 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Outcomes in patients with heart failure with preserved ejection fraction: it is more than the heart.J Am Coll Cardiol. 2012 Mar 13;59(11):1006-7. doi: 10.1016/j.jacc.2011.12.011. J Am Coll Cardiol. 2012. PMID: 22402072 No abstract available.
References
-
- Fonarow GC, Stough WG, Abraham WT, et al. Characteristics, treatments, and outcomes of patients with preserved systolic function hospitalized for heart failure: a report from the OPTIMIZE-HF Registry. J Am Coll Cardiol. 2007;50:768–77. - PubMed
-
- Yancy CW, Lopatin M, Stevenson LW, De MT, Fonarow GC. Clinical presentation, management, and in-hospital outcomes of patients admitted with acute decompensated heart failure with preserved systolic function: a report from the Acute Decompensated Heart Failure National Registry (ADHERE) Database. J Am Coll Cardiol. 2006;47:76–84. - PubMed
-
- Hogg K, Swedberg K, McMurray J. Heart failure with preserved left ventricular systolic function; epidemiology, clinical characteristics, and prognosis. J Am Coll Cardiol. 2004;43:317–27. - PubMed
-
- Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 2006;355:251–9. - PubMed
-
- Senni M, Redfield MM. Heart failure with preserved systolic function. A different natural history? J Am Coll Cardiol. 2001;38:1277–82. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
