

Target repositional accuracy and PTV margin verification using three-dimensional cone-beam computed tomography (CBCT) in stereotactic body radiotherapy (SBRT) of lung cancers
- PMID: 22402387
- PMCID: PMC5716422
- DOI: 10.1120/jacmp.v13i2.3708
Target repositional accuracy and PTV margin verification using three-dimensional cone-beam computed tomography (CBCT) in stereotactic body radiotherapy (SBRT) of lung cancers
Abstract
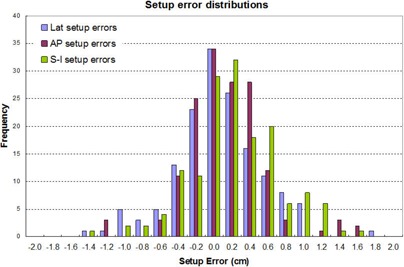
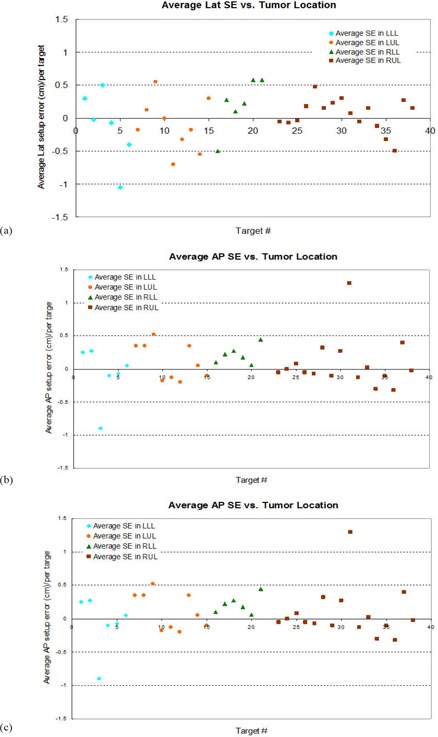
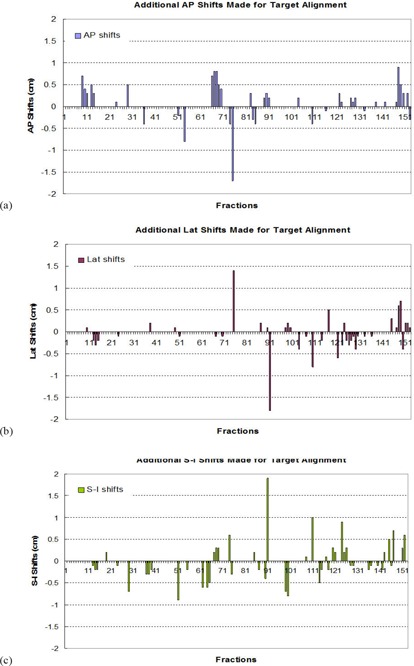
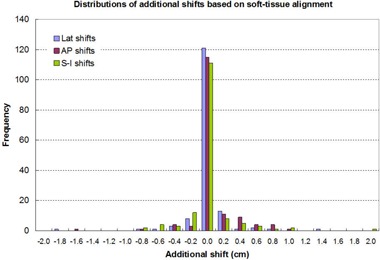
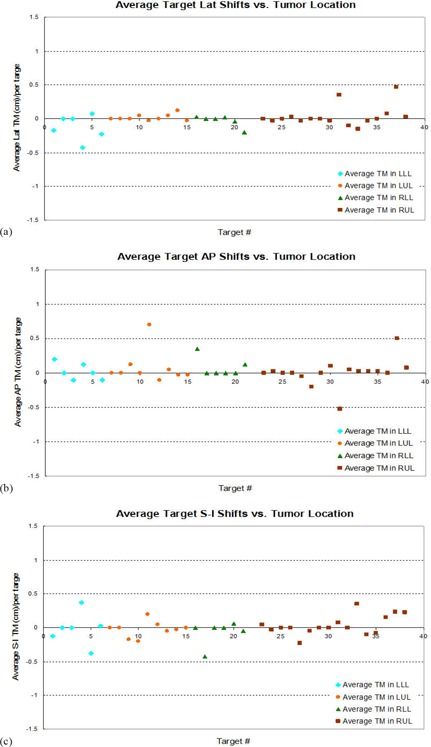
The purpose of this study was to assess target repositional accuracy with respect to the bony structures using daily CBCT, and to validate the planning target volume (PTV) margin used in the lung SBRT. All patients underwent 4D CT scanning in preparation for lung SBRT. The internal target volume (ITV) was outlined from the reconstructed 4D data using the maximum-intensity projection (MIP) algorithm. A 6 mm margin was added to the ITV to create the PTV. Conformal treatment planning was performed on the helical images, to which the MIP images were fused. Prior to each treatment, CBCT was taken after a patient was set up in the treatment position. The CBCT images were fused with the simulation CT based on the bony anatomy, in order to derive setup errors and separate them from the tumor repositional errors. The treating physician then checked and modified the alignment based on target relocalization within the PTV. The shifts determined in such a method were recorded and the subtractions of these shifts with respect to the corresponding setup errors were defined as the target relocalization accuracy. Our study of 36 consecutive patients, treating 38 targets for a total of 153 fractions shows that, after setup error correction, the target repositional accuracy followed a normal distribution with the mean values close to 0 in all directions, and standard deviations of 0.25 cm in A-P, 0.24 cm in Lat, and 0.28 cm in S-I directions, respectively. The probability of having the shifts ? 0.6 cm is less than 0.8% in A-P, 0.6% in Lat, and 1.7 % in S-I directions. For the patient population studied, the target centroid position relative to the bony structures changed minimally from day to day. This demonstrated that the PTV margin that is designed on the MIP image-based ITV was adequate for lung SBRT.
Figures


Similar articles
-
Evaluation of interfractional variation of the centroid position and volume of internal target volume during stereotactic body radiotherapy of lung cancer using cone-beam computed tomography.J Appl Clin Med Phys. 2016 Mar 8;17(2):461-472. doi: 10.1120/jacmp.v17i2.5835. J Appl Clin Med Phys. 2016. PMID: 27074466 Free PMC article.
-
Verification of planning target volume settings in volumetric modulated arc therapy for stereotactic body radiation therapy by using in-treatment 4-dimensional cone beam computed tomography.Int J Radiat Oncol Biol Phys. 2013 Jul 1;86(3):426-31. doi: 10.1016/j.ijrobp.2013.02.019. Epub 2013 Apr 5. Int J Radiat Oncol Biol Phys. 2013. PMID: 23562767
-
SU-E-J-24: Image-Guidance Using Cone-Beam CT for Stereotactic Body Radiotherapy (SBRT) of Lung Cancer Patients: Bony Alignment or Soft Tissue Alignment?Med Phys. 2012 Jun;39(6Part6):3657. doi: 10.1118/1.4734857. Med Phys. 2012. PMID: 28517596
-
ITV versus mid-ventilation for treatment planning in lung SBRT: a comparison of target coverage and PTV adequacy by using in-treatment 4D cone beam CT.Radiat Oncol. 2020 Mar 3;15(1):54. doi: 10.1186/s13014-020-01496-5. Radiat Oncol. 2020. PMID: 32127010 Free PMC article.
-
Evaluation of the cone beam CT for internal target volume localization in lung stereotactic radiotherapy in comparison with 4D MIP images.Med Phys. 2013 Nov;40(11):111709. doi: 10.1118/1.4823785. Med Phys. 2013. PMID: 24320417
Cited by
-
A block matching-based registration algorithm for localization of locally advanced lung tumors.Med Phys. 2014 Apr;41(4):041704. doi: 10.1118/1.4867860. Med Phys. 2014. PMID: 24694124 Free PMC article.
-
A phantom-based analysis for tracking intra-fraction pancreatic tumor motion by ultrasound imaging during radiation therapy.Front Oncol. 2022 Sep 27;12:996537. doi: 10.3389/fonc.2022.996537. eCollection 2022. Front Oncol. 2022. PMID: 36237341 Free PMC article.
-
Accuracy of automatic matching of Catphan 504 phantom in cone-beam computed tomography for tube current-exposure time product.J Appl Clin Med Phys. 2016 Nov 8;17(6):421-428. doi: 10.1120/jacmp.v17i6.6402. J Appl Clin Med Phys. 2016. PMID: 27929513 Free PMC article.
-
Assessment of setup uncertainties for various tumor sites when using daily CBCT for more than 2200 VMAT treatments.J Appl Clin Med Phys. 2014 Mar 6;15(2):4418. doi: 10.1120/jacmp.v15i2.4418. J Appl Clin Med Phys. 2014. PMID: 24710431 Free PMC article.
-
Spine Stereotactic Body Radiation Therapy Residual Setup Errors and Intra-Fraction Motion Using the Stereotactic X-Ray Image Guidance Verification System.Int J Med Phys Clin Eng Radiat Oncol. 2014 Feb;3(1):1-8. doi: 10.4236/ijmpcero.2014.31001. Int J Med Phys Clin Eng Radiat Oncol. 2014. PMID: 29333353 Free PMC article.
References
-
- Shimizu S, Shirato H, Kagei K, et al. Impact of respiratory movement on the computed tomographic images of small lung tumors in three‐dimensional (3D) radiotherapy. Int J Radiat Oncol Biol Phys. 2000; 46 (5): 1127–33. - PubMed
-
- Seppenwoolde Y, Shirato H, Kitamura K, et al. Precise and real‐time measurement of 3D tumor motion in lung due to breathing and heartbeat, measured during radiotherapy. Int J Radiat Oncol Biol Phys. 2002; 53 (4): 822–34. - PubMed
-
- Shirato H, Seppenwoolde Y, Kitamura K, Onimura R, Shimizu S. Intrafractional tumor motion: lung and liver. Semin Radiat Oncol. 2004; 14 (1): 10–18. - PubMed
-
- Sixel KE, Ruschin M, Tirona R, Cheung PC. Digital fluoroscopy to quantify lung tumor motion: potential for patient‐specific planning target volumes. Int J Radiat Oncol Biol Phys. 2003; 57 (3): 717–23. - PubMed
-
- Stevens CW, Munden RF, Forster KM, et al. Respiratory‐driven lung tumor motion is independent of tumor size, tumor location, and pulmonary function. Int J Radiat Oncol Biol Phys. 2001; 51 (1): 62–68. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
