

Electronic tools to assist with identification and counseling for overweight patients: a randomized controlled trial
- PMID: 22402982
- PMCID: PMC3403149
- DOI: 10.1007/s11606-012-2022-8
Electronic tools to assist with identification and counseling for overweight patients: a randomized controlled trial
Abstract
Background: Physicians often do not recognize when their patients are overweight and infrequently counsel them about weight loss.
Objective: To evaluate a set of electronic health record (EHR)-embedded tools to assist with identification and counseling of overweight patients.
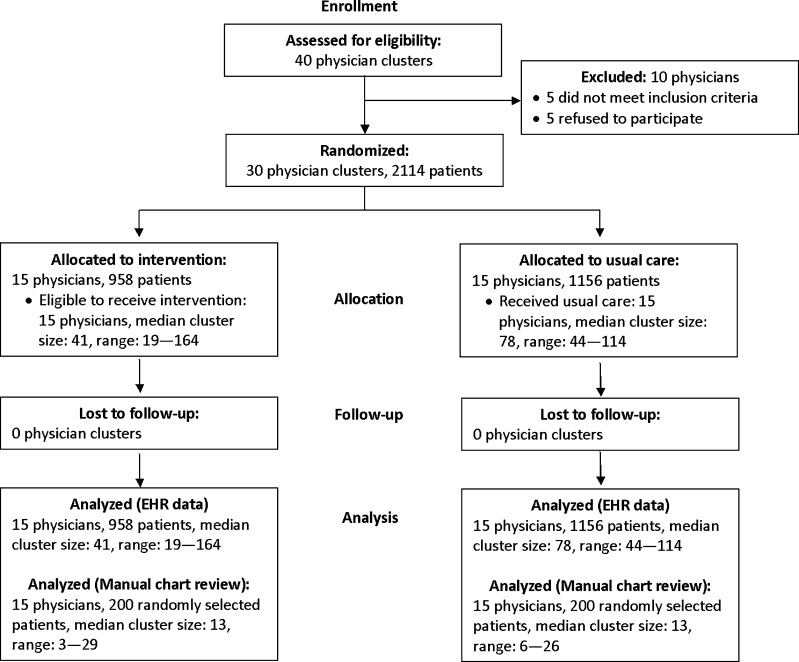
Design: Randomized controlled trial.
Participants: Physicians at an academic general internal medicine clinic were randomized to activation of the EHR tools (n = 15) or to usual care (n = 15). Patients of these physicians were included in analyses if they had a body mass index (BMI) between 27 and 29.9 kg/m(2).
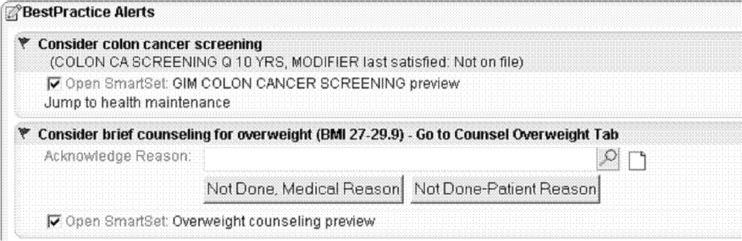
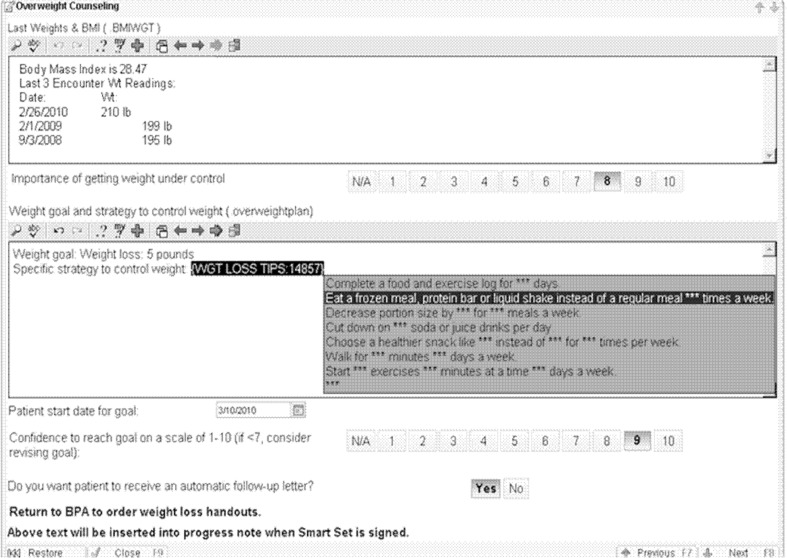
Intervention: The EHR tool set included: a physician point-of-care alert for overweight (BMI 27-29. 9 kg/m(2)); a counseling template to help physicians counsel patients on action plans; and an order set to facilitate entry of overweight as a diagnosis and to order relevant patient handouts.
Main measures: Physician documentation of overweight as a problem; documentation of weight-specific counseling; physician perceptions of the EHR tools; patient self-reported progress toward their goals and perspectives about counseling received.
Key results: Patients of physicians receiving the intervention were more likely than those of usual care physicians to receive a diagnosis of overweight (22% vs. 7%; p = 0.02) and weight-specific counseling (27% vs. 15%; p = 0.02). Most patients receiving counseling in the intervention group reported increased motivation to lose weight (90%) and taking steps toward their goal (93%). Most intervention physicians agreed that the tool alerted them to patients they did not realize were overweight (91%) and improved the effectiveness of their counseling (82%); more than half (55%) reported counseling overweight patients more frequently (55%). However, most physicians used the tool infrequently because of time barriers.
Conclusions: EHR-based alerts and management tools increased documentation of overweight and counseling frequency; the majority of patients for whom the tools were used reported short-term behavior change.
Figures

References
-
- McTigue KM, Garrett JM, Popkin BM. The natural history of the development of obesity in a cohort of young U.S. adults between 1981 and 1998. Ann Intern Med. 2002;136(12):857–864. - PubMed
-
- McTigue KM, Harris R, Hemphill B, et al. Screening and interventions for obesity in adults: summary of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med. 2003;139(11):933–949. - PubMed
-
- Vasan RS, Pencina MJ, Cobain M, Freiberg MS, D'Agostino RB. Estimated risks for developing obesity in the Framingham Heart Study. Ann Intern Med. 2005;143(7):473–480. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
