

Mobile phone use and glioma risk: comparison of epidemiological study results with incidence trends in the United States
- PMID: 22403263
- PMCID: PMC3297541
- DOI: 10.1136/bmj.e1147
Mobile phone use and glioma risk: comparison of epidemiological study results with incidence trends in the United States
Abstract
Objective: In view of mobile phone exposure being classified as a possible human carcinogen by the International Agency for Research on Cancer (IARC), we determined the compatibility of two recent reports of glioma risk (forming the basis of the IARC's classification) with observed incidence trends in the United States.
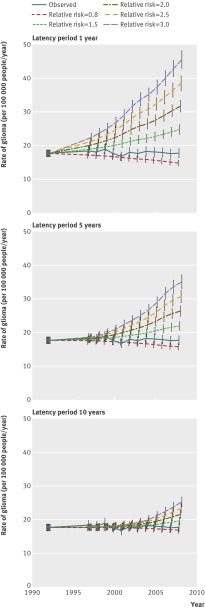
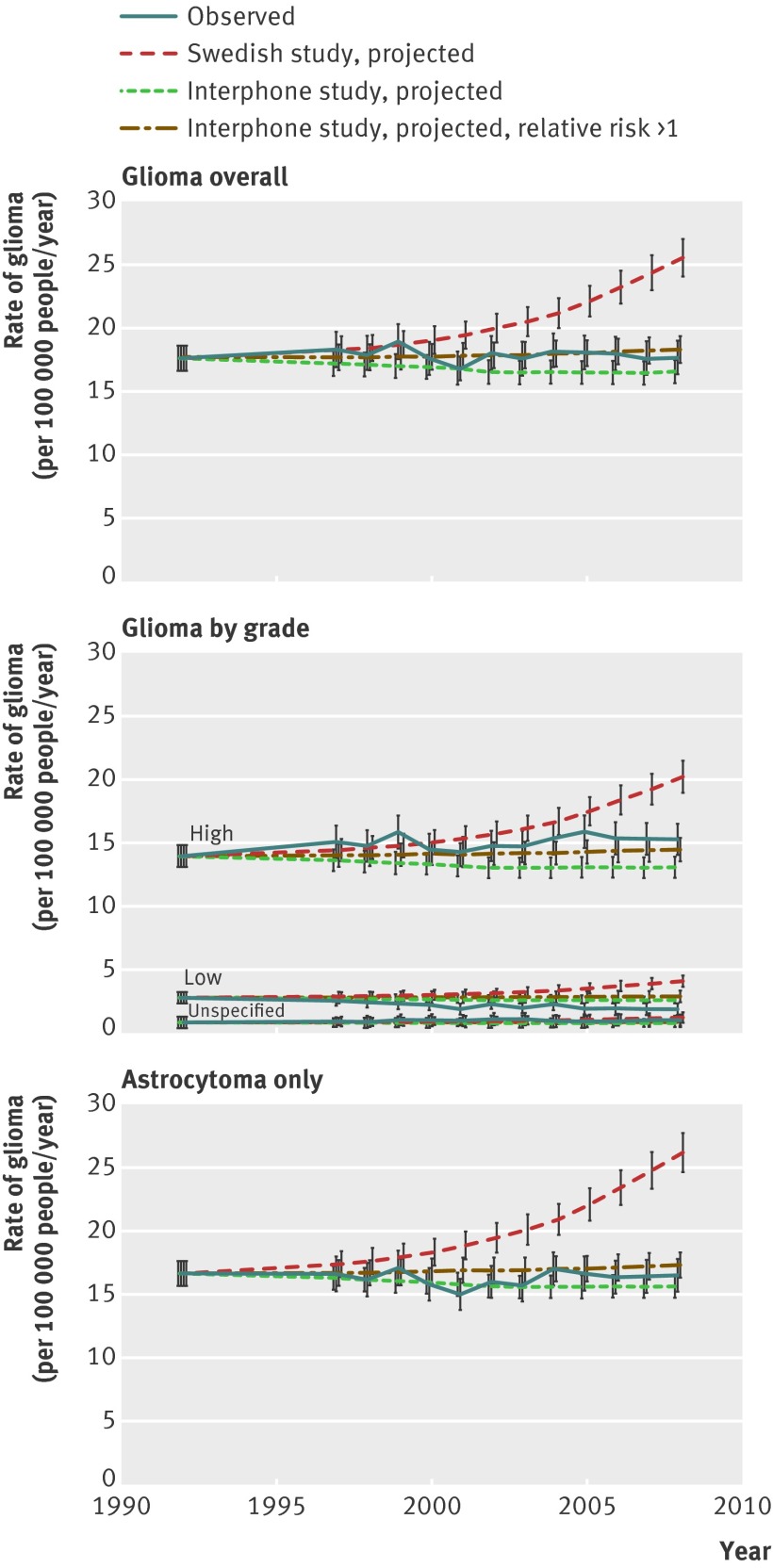
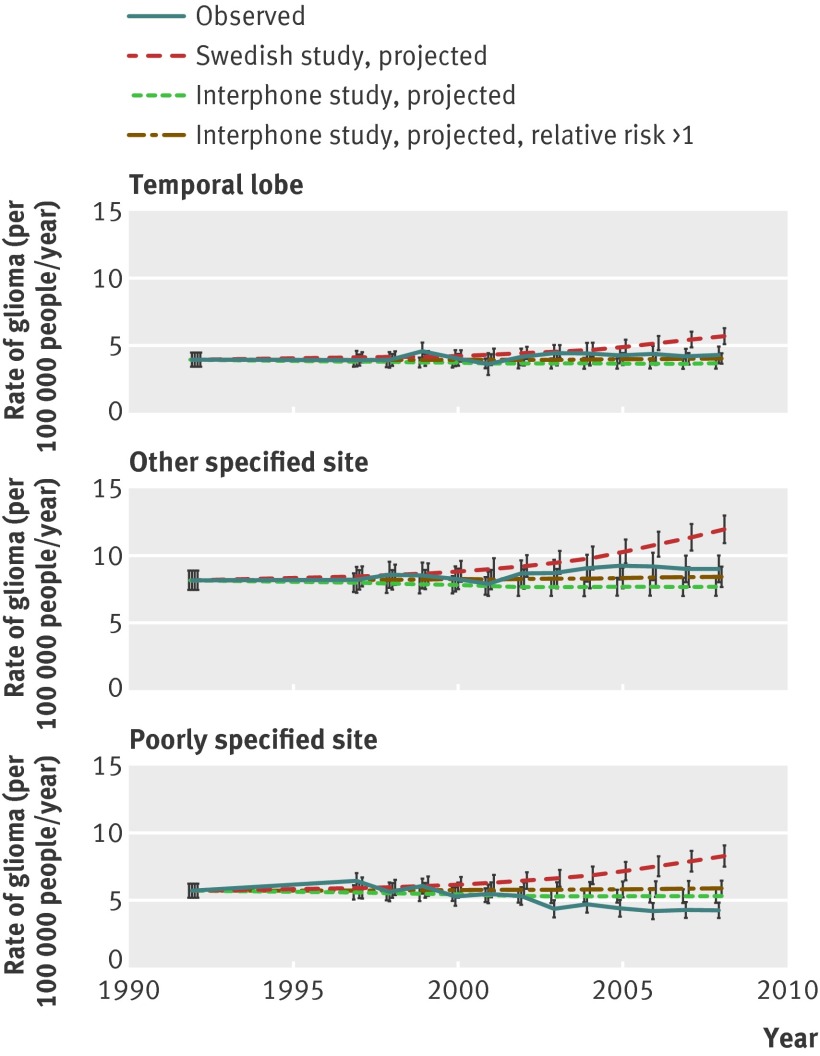
Design: Comparison of observed rates with projected rates of glioma incidence for 1997-2008. We estimated projected rates by combining relative risks reported in the 2010 Interphone study and a 2011 Swedish study by Hardell and colleagues with rates adjusted for age, registry, and sex; data for mobile phone use; and various latency periods.
Setting: US population based data for glioma incidence in 1992-2008, from 12 registries in the Surveillance, Epidemiology, and End Results (SEER) programme (Atlanta, Detroit, Los Angeles, San Francisco, San Jose-Monterey, Seattle, rural Georgia, Connecticut, Hawaii, Iowa, New Mexico, and Utah).
Participants: Data for 24,813 non-Hispanic white people diagnosed with glioma at age 18 years or older.
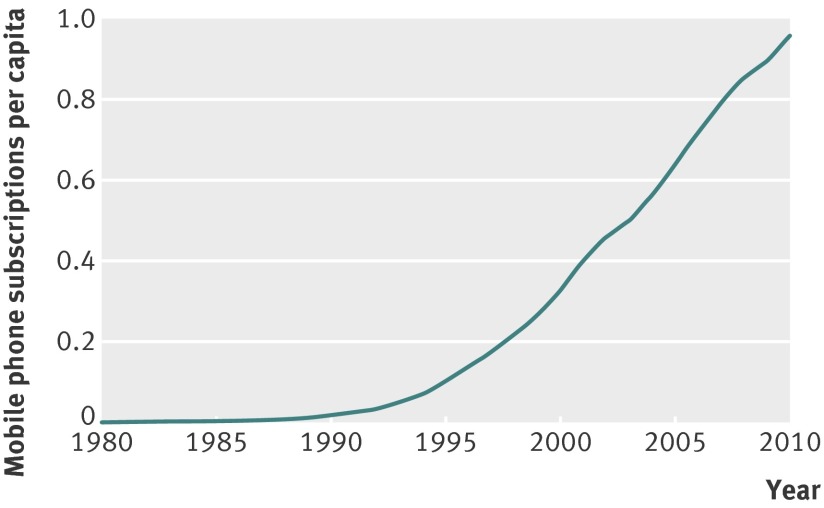
Results: Age specific incidence rates of glioma remained generally constant in 1992-2008 (-0.02% change per year, 95% confidence interval -0.28% to 0.25%), a period coinciding with a substantial increase in mobile phone use from close to 0% to almost 100% of the US population. If phone use was associated with glioma risk, we expected glioma incidence rates to be higher than those observed, even with a latency period of 10 years and low relative risks (1.5). Based on relative risks of glioma by tumour latency and cumulative hours of phone use in the Swedish study, predicted rates should have been at least 40% higher than observed rates in 2008. However, predicted glioma rates based on the small proportion of highly exposed people in the Interphone study could be consistent with the observed data. Results remained valid if we used either non-regular users or low users of mobile phones as the baseline category, and if we constrained relative risks to be more than 1.
Conclusions: Raised risks of glioma with mobile phone use, as reported by one (Swedish) study forming the basis of the IARC's re-evaluation of mobile phone exposure, are not consistent with observed incidence trends in US population data, although the US data could be consistent with the modest excess risks in the Interphone study.
Figures
Comment in
-
Study of mobile phone use and glioma risk was fatally flawed.BMJ. 2012 May 1;344:e3078; author reply e3088. doi: 10.1136/bmj.e3078. BMJ. 2012. PMID: 22549064 No abstract available.
-
Association of mobile phone use with adult brain cancer remains plausible.BMJ. 2012 May 1;344:e3083; author reply e3088. doi: 10.1136/bmj.e3083. BMJ. 2012. PMID: 22549065 No abstract available.
References
-
- Muscat JE, Malkin MG, Thompson S, Shore RE, Stellman SD, McRee D, et al. Handheld cellular telephone use and risk of brain cancer. JAMA 2000;284:3001-7. - PubMed
-
- Inskip PD, Tarone RE, Hatch EE, Wilcosky TC, Shapiro WR, Selker RG, et al. Cellular-telephone use and brain tumors. N Engl J Med 2001;344:79-86. - PubMed
-
- Schüz J, Jacobsen R, Olsen JH, Boice JD Jr, McLaughlin JK, Johansen C. Cellular telephone use and cancer risk: update of a nationwide Danish cohort. J Natl Cancer Inst 2006;98:1707-13. - PubMed
-
- INTERPHONE Study Group. Brain tumour risk in relation to mobile telephone use: results of the INTERPHONE international case-control study. Int J Epidemiol 2010;39:675-94. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical