

Modifiable practices associated with sudden death among hemodialysis patients in the Dialysis Outcomes and Practice Patterns Study
- PMID: 22403271
- PMCID: PMC3338277
- DOI: 10.2215/CJN.08850811
Modifiable practices associated with sudden death among hemodialysis patients in the Dialysis Outcomes and Practice Patterns Study
Abstract
Background and objectives: Sudden death is common in hemodialysis patients, but whether modifiable practices affect the risk of sudden death remains unclear.
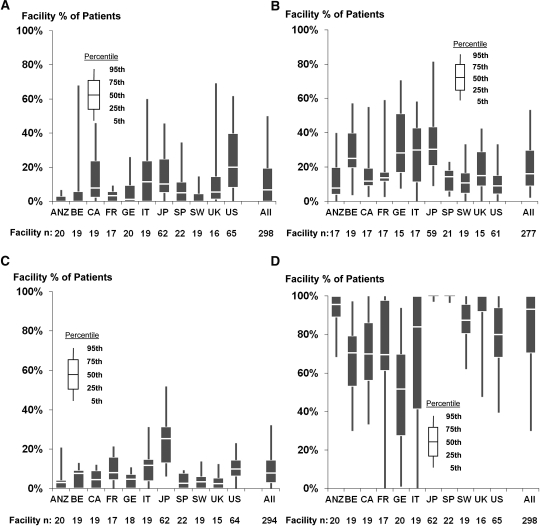
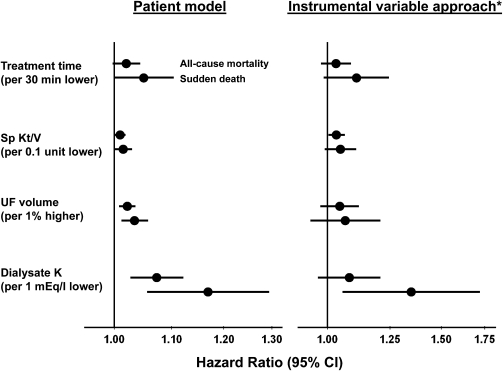
Design, setting, participants, & measurements: This study analyzed 37,765 participants in 12 countries in the Dialysis Outcomes and Practice Patterns Study to explore the association of the following practices with sudden death (due to cardiac arrhythmia, cardiac arrest, and/or hyperkalemia): treatment time [TT] <210 minutes, Kt/V <1.2, ultrafiltration volume >5.7% of postdialysis weight, low dialysate potassium [K(D) <3]), and prescription of Q wave/T wave interval-prolonging drugs. Cox regression was used to estimate effects on mortality, adjusting for potential confounders. An instrumental variable approach was used to further control for unmeasured patient-level confounding.
Results: There were 9046 deaths, 26% of which were sudden (crude mortality rate, 15.3/100 patient-years; median follow-up, 1.59 years). Associations with sudden death included hazard ratios of 1.13 for short TT, 1.15 for large ultrafiltration volume, and 1.10 for low Kt/V. Compared with K(D) ≥3 mEq/L, the sudden death rate was higher for K(D) ≤1.5 and K(D)=2-2.5 mEq/L. The instrumental variable approach yielded generally consistent findings. The sudden death rate was elevated for patients taking amiodarone, but not other Q wave/T wave interval-prolonging drugs.
Conclusions: This study identified modifiable dialysis practices associated with higher risk of sudden death, including short TT, large ultrafiltration volume, and low K(D). Because K(D) <3 mEq/L is common and easy to change, K(D) tailoring may prevent some sudden deaths. This hypothesis merits testing in clinical trials.
Figures

References
-
- Herzog CA, Mangrum JM, Passman R: Sudden cardiac death and dialysis patients. Semin Dial 21: 300–307, 2008 - PubMed
-
- Parekh RS, Plantinga LC, Kao WHL, Meoni LA, Jaar BG, Fink NE, Powe NR, Coresh J, Klag MJ: The association of sudden cardiac death with inflammation and other traditional risk factors. Kidney Int 74: 1335–1342, 2008 - PubMed
-
- Morrison G, Michelson EL, Brown S, Morganroth J: Mechanism and prevention of cardiac arrhythmias in chronic hemodialysis patients. Kidney Int 17: 811–819, 1980 - PubMed
-
- Bleyer AJ, Hartman J, Brannon PC, Reeves-Daniel A, Satko SG, Russell G: Characteristics of sudden death in hemodialysis patients. Kidney Int 69: 2268–2273, 2006 - PubMed
-
- Bleyer AJ, Russell GB, Satko SG: Sudden and cardiac death rates in hemodialysis patients. Kidney Int 55: 1553–1559, 1999 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
