

Multicytokine detection improves latent tuberculosis diagnosis in health care workers
- PMID: 22403417
- PMCID: PMC3347142
- DOI: 10.1128/JCM.00117-12
Multicytokine detection improves latent tuberculosis diagnosis in health care workers
Abstract
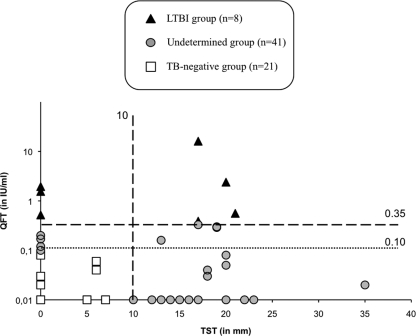
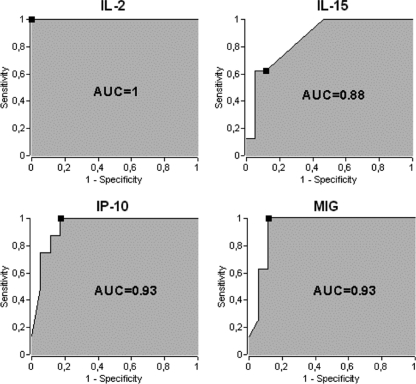
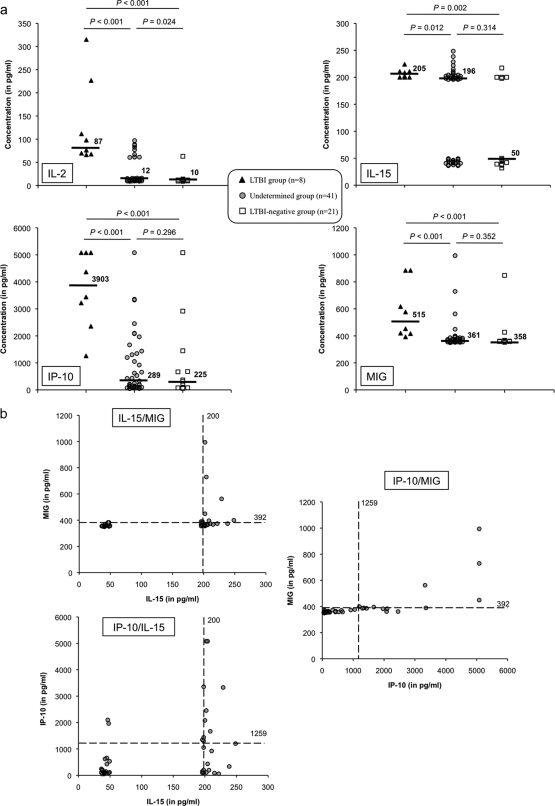
In a low-incidence setting, health care workers (HCW) are at a higher risk of tuberculosis than the general population. The suboptimal sensitivity of the QuantiFERON-TB Gold In-Tube (QFT) test remains a critical issue when identifying occupational latent tuberculosis infection (LTBI) in HCW. The aim of this study was to identify additional biomarkers in order to overcome the limits of gamma interferon (IFN-γ) release assays (IGRAs) and improve the performance of LTBI diagnosis within this population. Seventy Bacille Calmette-Guérin-vaccinated HCW regularly exposed to Mycobacterium tuberculosis were grouped according to QFT results into an LTBI-positive group (positive QFT, n = 8), an LTBI-negative group (normal QFT and negative tuberculin skin test [TST], n = 21), and an undetermined group (subpositive QFT and/or positive TST, n = 41). The secretion of 22 cytokines in response to QFT-specific stimulation was quantified using a multiparameter-based immunoassay. As a result, thresholds discriminating LTBI-positive from LTBI-negative HCW were established by comparing areas under the receiver operating characteristic curves for interleukin-2 (IL-2), IL-15, IFN-γ-induced protein 10 (IP-10), and the monokine induced by IFN-γ (MIG), which are biomarkers differentially secreted by the two groups. The combination of IL-15 and MIG provided a sensitivity of 100% and a specificity of 94.1% in distinguishing LTBI-positive from LTBI-negative HCW. When using IL-15 and MIG among the undetermined group, 6/45 HCW could be classified in the LTBI-positive group. The use of additional biomarkers after IGRA screening could improve the diagnosis of LTBI. The performance of these biomarkers and their use in combination with TST and/or QFT, as well as the cost-effectiveness of such a diagnostic strategy, should be evaluated in further larger clinical trials.
Figures

References
-
- Abramo C, et al. 2006. Monokine induced by interferon gamma and IFN-gamma response to a fusion protein of Mycobacterium tuberculosis ESAT-6 and CFP-10 in Brazilian tuberculosis patients. Microbes Infect. 8:45–51 - PubMed
-
- Andersen P, Munk ME, Pollock JM, Doherty TM. 2000. Specific immune-based diagnosis of tuberculosis. Lancet 356:1099–1104 - PubMed
-
- Anonymous 2006. Test de detection de la production d'interféron-gamma pour le diagnostic des infections tuberculeuses. Haute Autorité de Santé, Saint-Denis La Plaine, France: http://www.has-sante.fr/portail/upload/docs/application/pdf/synthese_det...
-
- Biselli R, et al. 2010. Detection of interleukin-2 in addition to interferon-gamma discriminates active tuberculosis patients, latently infected individuals, and controls. Clin. Microbiol. Infect. 16:1282–1284 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
