

Clinical Manifestations of Kaposi Sarcoma Herpesvirus Lytic Activation: Multicentric Castleman Disease (KSHV-MCD) and the KSHV Inflammatory Cytokine Syndrome
- PMID: 22403576
- PMCID: PMC3291870
- DOI: 10.3389/fmicb.2012.00073
Clinical Manifestations of Kaposi Sarcoma Herpesvirus Lytic Activation: Multicentric Castleman Disease (KSHV-MCD) and the KSHV Inflammatory Cytokine Syndrome
Erratum in
-
Corrigendum: Clinical manifestations of Kaposi sarcoma herpesvirus lytic activation: multicentric Castleman disease (KSHV-MCD) and the KSHV inflammatory cytokine syndrome.Front Microbiol. 2017 Aug 21;8:1572. doi: 10.3389/fmicb.2017.01572. eCollection 2017. Front Microbiol. 2017. PMID: 28845155 Free PMC article.
Abstract
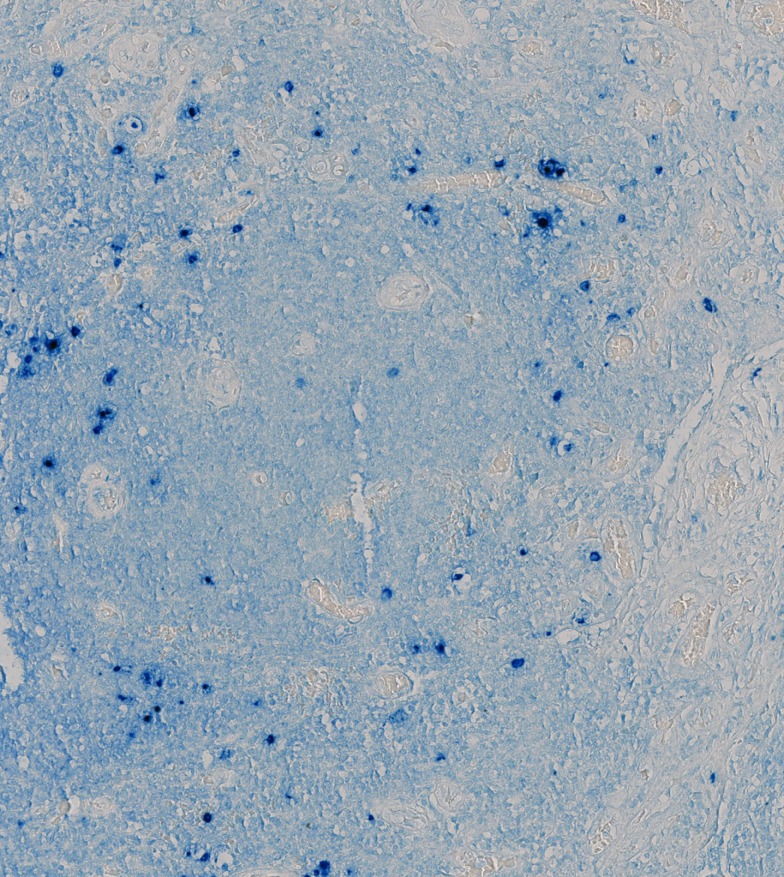
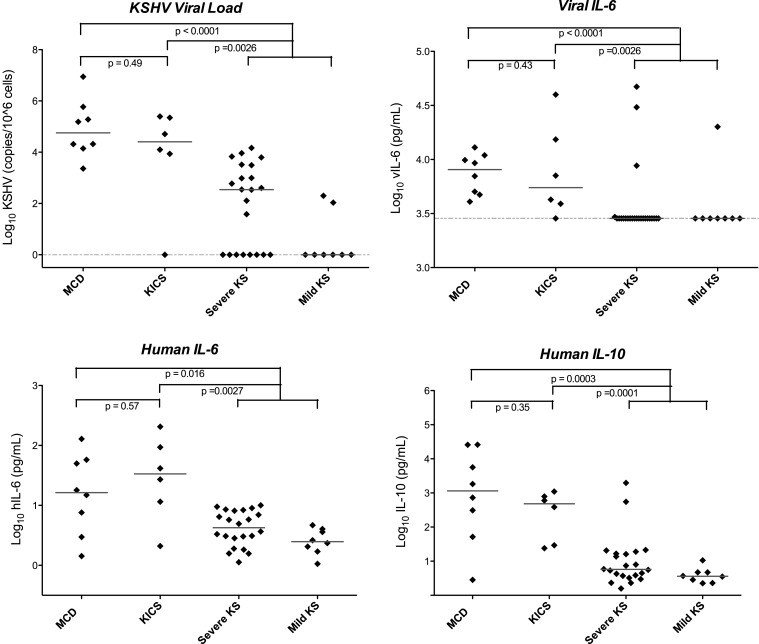
Soon after the discovery of Kaposi sarcoma (KS)-associated herpesvirus (KSHV), it was appreciated that this virus was associated with most cases of multicentric Castleman disease (MCD) arising in patients infected with human immunodeficiency virus. It has subsequently been recognized that KSHV-MCD is a distinct entity from other forms of MCD. Like MCD that is unrelated to KSHV, the clinical presentation of KSHV-MCD is dominated by systemic inflammatory symptoms including fevers, cachexia, and laboratory abnormalities including cytopenias, hypoalbuminemia, hyponatremia, and elevated C-reactive protein. Pathologically KSHV-MCD is characterized by polyclonal, IgM-lambda restricted plasmacytoid cells in the intrafollicular areas of affected lymph nodes. A portion of these cells are infected with KSHV and a sizable subset of these cells express KSHV lytic genes including a viral homolog of interleukin-6 (vIL-6). Patients with KSHV-MCD generally have elevated KSHV viral loads in their peripheral blood. Production of vIL-6 and induction of human (h) IL-6 both contribute to symptoms, perhaps in combination with overproduction of IL-10 and other cytokines. Until recently, the prognosis of patients with KSHV-MCD was poor. Recent therapeutic advances targeting KSHV-infected B cells with the anti-CD20 monoclonal antibody rituximab and utilizing KSHV enzymes to target KSHV-infected cells have substantially improved patient outcomes. Recently another KSHV-associated condition, the KSHV inflammatory cytokine syndrome (KICS) has been described. Its clinical manifestations resemble those of KSHV-MCD but lymphadenopathy is not prominent and the pathologic nodal changes of KSHV-MCD are absent. Patients with KICS exhibit elevated KSHV viral loads and elevation of vIL-6, homolog of human interleukin-6 and IL-10 comparable to those seen in KSHV-MCD; the cellular origin of these is a matter of investigation. KICS may contribute to the inflammatory symptoms seen in some patients with severe KS or primary effusion lymphoma. Additional research is needed to better define the clinical spectrum of KICS and its relationship to KSHV-MCD. In additional, research is needed to better understand the pathogenesis and epidemiology of both KICS and KSHV-MCD, as well as the optimal therapy for both of these disorders.
Keywords: KSHV inflammatory cytokine syndrome; Kaposi sarcoma-associated herpesvirus; human herpesvirus 8; human immunodeficiency virus; interleukin-6; multicentric Castleman disease.
Figures
References
-
- Abend J. R., Uldrick T., Ziegelbauer J. M. (2010). Regulation of tumor necrosis factor-like weak inducer of apoptosis receptor protein (TWEAKR) expression by Kaposi’s sarcoma-associated herpesvirus microRNA prevents TWEAK-induced apoptosis and inflammatory cytokine expression. J. Virol. 84, 12139–12151. 10.1128/JVI.00884-10 - DOI - PMC - PubMed
-
- Ayers L. W., Lukande R., NDung’u J. R., Chumba D. K., Turnwine L. K. (2011). “Multicentric Castleman’s disease (MCD) and other related KSHV lymphoproliferations in East Africa,” in International Conference on Malignancies in AIDS and Other Acquired Immunodeficiencies, Bethesda, MD.
LinkOut - more resources
Full Text Sources
Research Materials