

Early non-invasive ventilation treatment for severe influenza pneumonia
- PMID: 22404211
- PMCID: PMC7128378
- DOI: 10.1111/j.1469-0691.2012.03797.x
Early non-invasive ventilation treatment for severe influenza pneumonia
Abstract
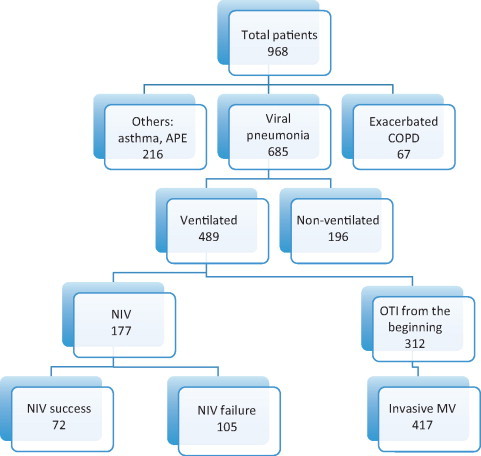
The role of non-invasive ventilation (NIV) in acute respiratory failure caused by viral pneumonia remains controversial. Our objective was to evaluate the use of NIV in a cohort of (H1N1)v pneumonia. Usefulness and success of NIV were assessed in a prospective, observational registry of patients with influenza A (H1N1) virus pneumonia in 148 Spanish intensive care units (ICUs) in 2009-10. Significant variables for NIV success were included in a multivariate analysis. In all, 685 patients with confirmed influenza A (H1N1)v viral pneumonia were admitted to participating ICUs; 489 were ventilated, 177 with NIV. The NIV was successful in 72 patients (40.7%), the rest required intubation. Low Acute Physiology and Chronic Health Evaluation (APACHE) II, low Sequential Organ Failure Assessment (SOFA) and absence of renal failure were associated with NIV success. Success of NIV was independently associated with fewer than two chest X-ray quadrant opacities (OR 3.5) and no vasopressor requirement (OR 8.1). However, among patients with two or more quadrant opacities, a SOFA score ≤7 presented a higher success rate than those with SOFA score >7 (OR 10.7). Patients in whom NIV was successful required shorter ventilation time, shorter ICU stay and hospital stay than NIV failure. In patients in whom NIV failed, the delay in intubation did not increase mortality (26.5% versus 24.2%). Clinicians used NIV in 25.8% of influenza A (H1N1)v viral pneumonia admitted to ICU, and treatment was effective in 40.6% of them. NIV success was associated with shorter hospital stay and mortality similar to non-ventilated patients. NIV failure was associated with a mortality similar to those who were intubated from the start.
© 2012 The Authors. Clinical Microbiology and Infection © 2012 European Society of Clinical Microbiology and Infectious Diseases.
Figures
References
-
- Lee N, Hui D, Wu A. A major outbreak of SARS in Hong Kong. N Engl J Med. 2003;348:1986–1994. - PubMed
-
- Jain S, Kamimoto L, Bramley AM. Hospitalized patients with 2009 H1N1 influenza in the United States, April–June 2009. N Engl J Med. 2009;361:1935–1944. - PubMed
-
- Domínguez‐Cherit G, Lapinsky SE, Macias AE. Critically ill patients with 2009 Influenza A (H1N1) in Mexico. JAMA. 2009;302:1880–1887. - PubMed
-
- Kumar A, Zarychanski R, Pinto R. Critically ill patients with 2009 Influenza A (H1N1) infection in Canada. JAMA. 2009;302:1872–1879. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
