

Keeping participants on board: increasing uptake by automated respondent reminders in an Internet-based chlamydia screening in the Netherlands
- PMID: 22404911
- PMCID: PMC3353245
- DOI: 10.1186/1471-2458-12-176
Keeping participants on board: increasing uptake by automated respondent reminders in an Internet-based chlamydia screening in the Netherlands
Abstract
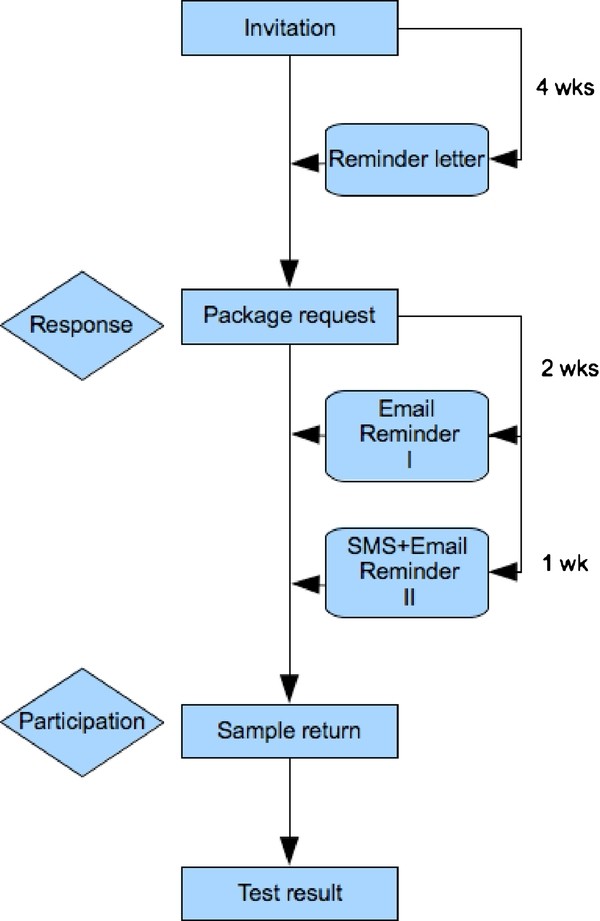
Background: Effectiveness of Chlamydia screening programs is determined by an adequate level of participation and the capturing of high-risk groups. This study aimed to evaluate the contribution of automated reminders by letter, email and short message service (SMS) on package request and sample return in an Internet-based Chlamydia screening among people aged 16 to 29 years in the Netherlands.
Methods: Individuals not responding to the invitation letter received a reminder letter after 1 month. Email- and SMS-reminders were sent to persons who did not return their sample. It was examined to what extent reminders enhanced the response rate (% of package requests) and participation rate (% of sample return). Sociodemographic and behavioural correlates of providing a cell phone number and participation after the reminder(s) were studied by logistic regression models.
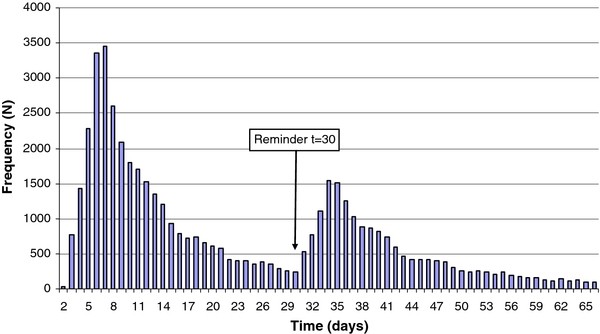
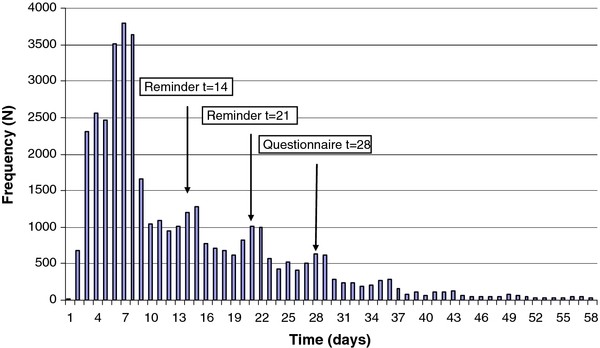
Results: Of all respondents (screening round 1: 52,628, round 2: 41,729), 99% provided an email address and 72% a cell phone number. Forty-two percent of all package requests were made after the reminder letter. The proportion of invitees returning a sample increased significantly from 10% to 14% after email/SMS reminders (round 2: from 7% to 10%). Determinants of providing a cell-phone number were younger age (OR in 25-29 year olds versus 16-19 year olds = 0.8, 95%CI 0.8-0.9), non-Dutch (OR in Surinam/Antillean versus Dutch = 1.3, 95%CI 1.2-1.4, Turkish/Moroccan: 1.1, 95%CI 1.0-1.2, Sub Sahara African: 1.5, 95%CI 1.3-1.8, non-Western other 1.1, 95%CI 1.1-1.2), lower educational level (OR in high educational level versus low level = 0.8, 95%CI 0.7-0.9), no condom use during the last contact with a casual partner (OR no condom use versus condom use 1.2, 95%CI 1.1-1.3), younger age at first sexual contact (OR 19 years or older versus younger than 16: 0.7, 95%CI 0.6-0.8). Determinants for requesting a test-package after the reminder letter were male gender (OR female versus male 0.9 95%CI 0.8-0.9), non-Dutch (OR in Surinam/Antillean versus Dutch 1.3, 95%CI 1.2-1.4, Turkish/Moroccan: 1.4, 95%CI 1.3-1.5, Sub Sahara African: 1.4, 95%CI 1.2-1.5, non-Western other: 1.2, 95%CI 1.1-1.2), having a long-term steady partnership (long-term versus short-term.1.2 95%CI 1.1-1.3). Email/SMS reminders seem to have resulted in more men and people aged 25-29 years returning a sample.
Conclusions: Nearly all respondents (99.5%) were reachable by modern communication media. Response and participation rates increased significantly after the reminders. The reminder letters also seemed to result in reaching more people at risk. Incorporation of automated reminders in Internet-based (Chlamydia) screening programs is strongly recommended.
Figures
References
-
- Op de Coul ELM, Weenen TC, van der Sande MAB, van den Broek IVF. RIVM Report 210261006. Bilthoven; 2009. Process evaluation of the Chlamydia Screening Implementation in the Netherlands: phase 1. Challenges and opportunities during preparation and first operational phase.
-
- van Bergen JEAM, Fennema JSA, van den Broek IVF, Brouwers EEHG, de Feijter EM, Hoebe CJPA, Koekenbier RH, de Coul ELM Op, van Ravesteijn SM, Götz HM. Rationale, design, and results of the first screening round of a comprehensive, register-based. Chlamydia screening implementation programme in the Netherlands. BMC Infect Dis. 2010;10:293. doi: 10.1186/1471-2334-10-293. - DOI - PMC - PubMed
-
- van den Broek IVF, Hoebe CJPA, van Bergen JEAM, Brouwers EEHG, de Feijter EM, Fennema JSA, Götz HM, Koekenbier RH, van Ravesteijn SM, Op de Coul ELM. Evaluation design of a systematic, selective, Internet-based Chlamydia Screening Implementation in the Netherlands, 2008-2010: implications of first results for the analysis. BMC Infect Dis. 2010;10:89. doi: 10.1186/1471-2334-10-89. - DOI - PMC - PubMed
-
- Greenland KE, Op de Coul ELM, van Bergen JEAM, Brouwers EEHG, Fennema JSA, Götz HM, Hoebe CJPA, Koekenbier RH, Pars LL, van Ravesteijn SM, van den Broek IVF. Acceptability of the internet-based Chlamydia Screening Implementation in the Netherlands and insights into non-response. Sex Transm Dis. 2011;38(6):467–474. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
