

Herlyn-Werner-Wunderlich syndrome: MRI findings, radiological guide (two cases and literature review), and differential diagnosis
- PMID: 22405336
- PMCID: PMC3314562
- DOI: 10.1186/1471-2342-12-4
Herlyn-Werner-Wunderlich syndrome: MRI findings, radiological guide (two cases and literature review), and differential diagnosis
Abstract
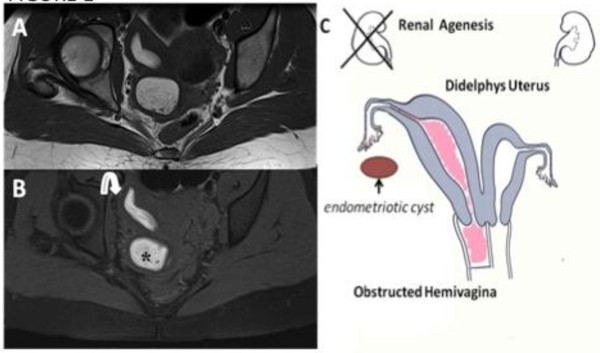
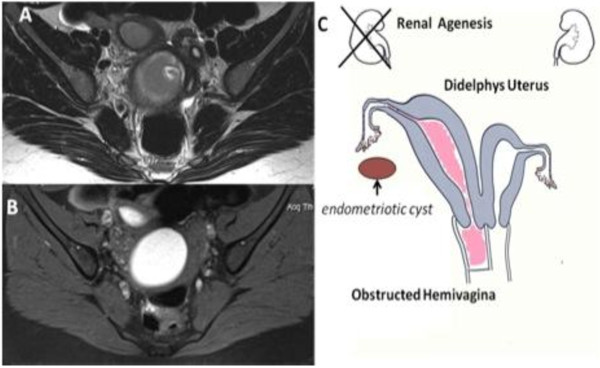
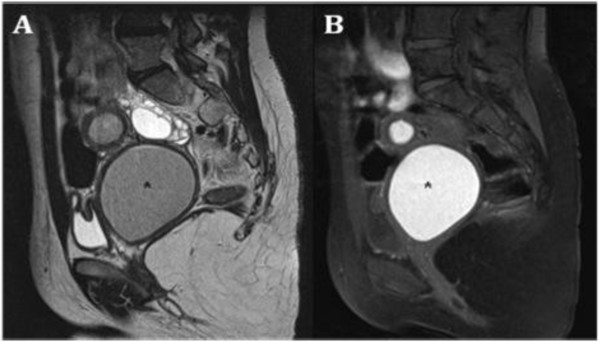
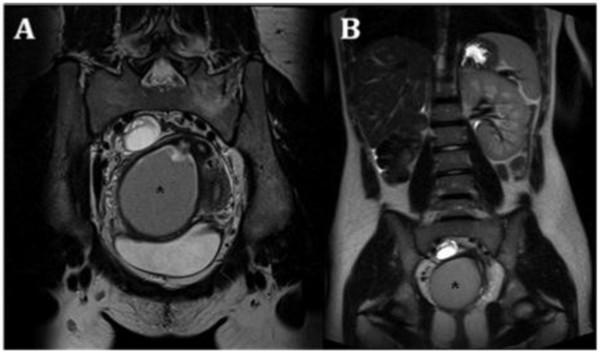
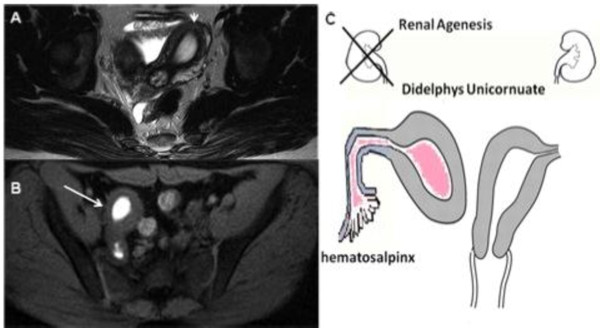
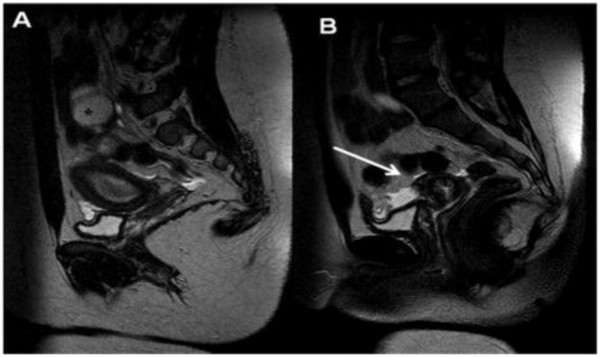
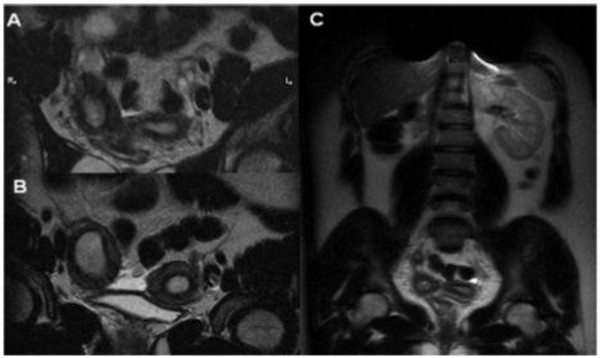
Background: Herlyn-Werner-Wunderlich (HWW) syndrome is a very rare congenital anomaly of the urogenital tract involving Müllerian ducts and Wolffian structures, and it is characterized by the triad of didelphys uterus, obstructed hemivagina and ipsilateral renal agenesis. It generally occurs at puberty and exhibits non-specific and variable symptoms with acute or pelvic pain shortly following menarche, causing a delay in the diagnosis. Moreover, the diagnosis is complicated by the infrequency of this syndrome, because Müllerian duct anomalies (MDA) are infrequently encountered in a routine clinical setting.
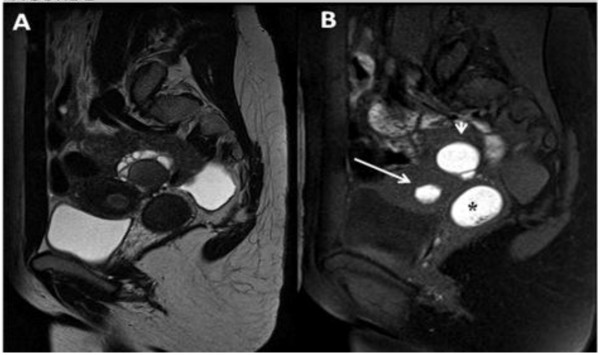
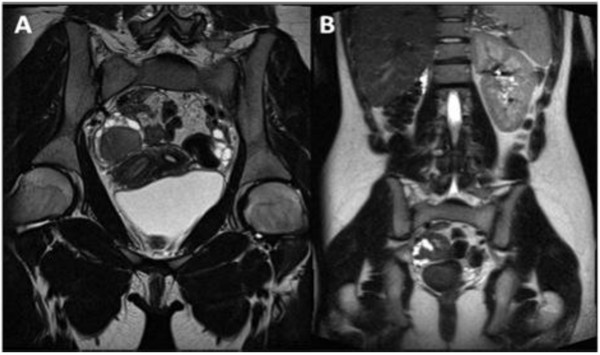
Cases presentation: two cases of HWW syndrome in adolescents and a differential diagnosis for one case of a different MDA, and the impact of magnetic resonance (MR) imaging technology to achieve the correct diagnosis.
Conclusions: MR imaging is a very suitable diagnostic tool in order to perform the correct diagnosis of HWW syndrome.
Figures
References
-
- Alan JW, Louis RK. Campbell-Walsh Urology. 9. Philadelphia: Saunders; pp. 3270–6.
-
- Lee BH, Kim JW, Oh SI. et al.3 cases of uterus didelphys with obstructed hemivagina and ipsilateral renal agenesis. Korean J Obstet Gynecol. 1997;40:1489–95.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
