

Trichoscopy update 2011
- PMID: 22408709
- PMCID: PMC3241952
- DOI: 10.3315/jdcr.2011.1083
Trichoscopy update 2011
Abstract
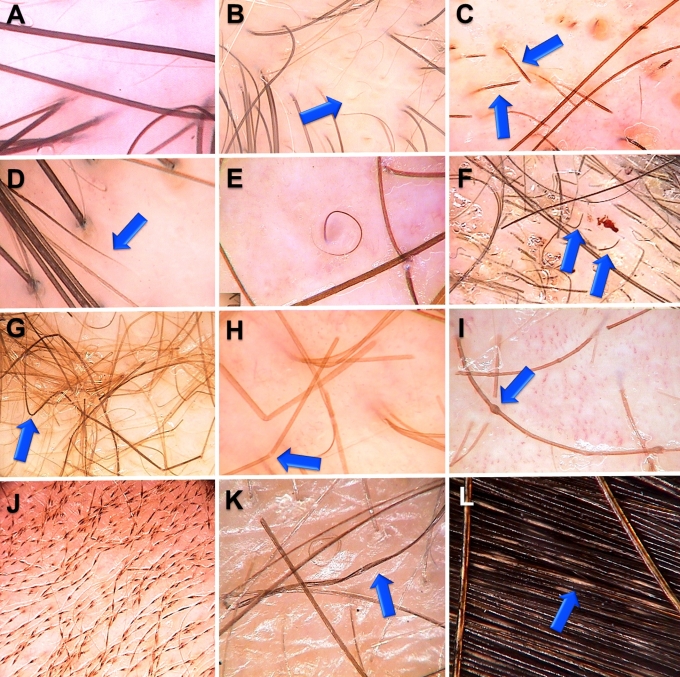
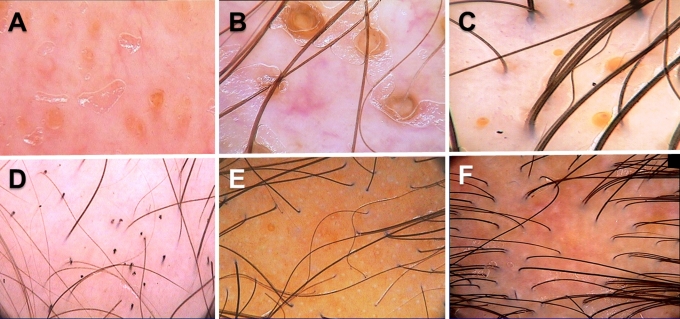
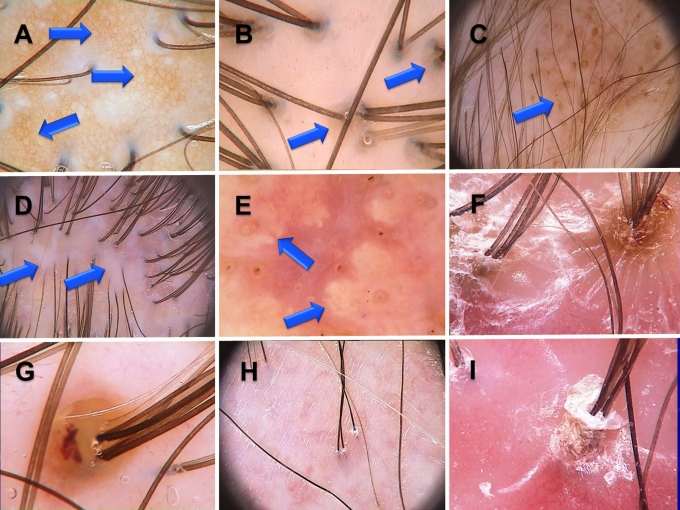
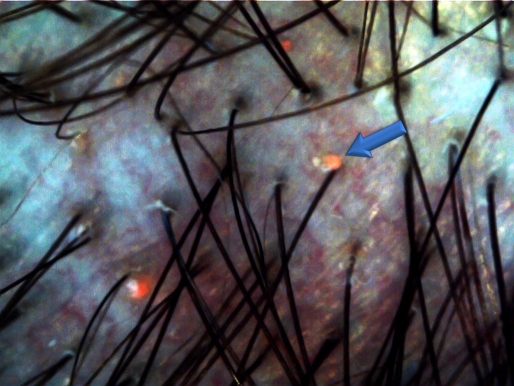
Trichoscopy performed with a handheld dermoscope or a videodermoscope became an indispensable tool in differential diagnosis of hair and scalp diseases. Current research is focusing on trichoscopy of: 1) non-cicatricial alopecia, 2) cicatricial alopecia, 3) hair shaft disorders, and 4) inflammatory scalp diseases. This review summarizes current knowledge in these four fields of research. In all non-cicatricial alopecias presence of empty follicular openings is a common trichoscopy finding. In alopecia areata black dots and micro-exclamation mark hairs and tapered hairs correlate with disease activity, whereas yellow dots and vellus hairs correlate with disease severity. In androgenic alopecia trichoscopy shows hair shaft thickness heterogeneity, multiple thin and vellus hairs, yellow dots, perifollicular discoloration, and predominance of follicular units with only one hair. These features predominate in the frontal area. In all forms of cicatricial alopecia, trichoscopy shows milky-red or ivory-white areas lacking follicular openings. In classic lichen planopilaris trichoscopy shows perifollicular inflammation, tubular perifollicular scaling, elongated, concentric blood vessels and "classic white dots", which merge to form white areas. Frontal fibrosing alopecia shows mild perifollicular scaling. Folliculitis decalvans is characterized by tufted hairs, large follicular pustules with emerging hair shafts and perifollicular starburst pattern hyperplasia. In dissecting cellulitis characteristic findings are "3D" yellow dots imposed over dystrophic hairs, large, yellow amorphous areas and pinpoint white dots with a whitish halo. Trichoscopy is particularly useful to diagnose hair shaft abnormalities in trichorrhexis nodosa, trichorrhexis invaginata, monilethrix, pili torti, and pili annulati. The method may be also useful in diagnosing inflammatory scalp diseases. In discoid lupus erythematosus trichoscopy shows large arborizing vessels and large hyperkeratotic folliculilar yellow dots. Trichoscopy of scalp psoriasis shows regularly distributed twisted and lacelike blood vessels, whereas in seborroic dermatitis thin arborizing vessels may be observed. In tinea capitis trichoscopy shows comma, corkscrew and zigzag hairs. Examination tinea capitis may be facilitated by UV-light enhanced trichoscopy (UVET). In conclusion, trichoscopy is a non-invasive method which may be applied in differential diagnosis of most hair and scalp diseases.
Keywords: UV; alopecia; dermoscopy; hair; lichen planopilaris; lupus; psoriasis; seborheic dermatitis; trichoscopy; videodermoscopy.
Figures
References
-
- Rudnicka L, Olszewska M, Rakowska A, Kowalska-Oledzka E, Slowinska M. Trichoscopy: a new method for diagnosing hair loss. J Drugs Dermatol. 2008;7:651–654. - PubMed
-
- Vogt A, McElwee KJ, Blume-Peytavi U. Biology of the hair follicle. In: Blume-Peytavi U, Tosti A, Whiting D, Trüeb R (Eds), Hair; from basic science to clinical application. Berlin, Germany: Springer-Verlag; 2008. pp. 1–22.
-
- Wagner R, Joekes I. Hair medulla morphology and mechanical properties. J Cosmet Sci. 2007;58:359–368. - PubMed
-
- Inui S, Nakajima T, Itami S. Scalp dermoscopy of androgenetic alopecia in Asian people. J Dermatol. 2009;36:82–85. - PubMed
LinkOut - more resources
Full Text Sources
Medical