

Disparities in receipt of antiretroviral therapy among HIV-infected adults (2002-2008)
- PMID: 22410406
- PMCID: PMC3779806
- DOI: 10.1097/MLR.0b013e31824e3356
Disparities in receipt of antiretroviral therapy among HIV-infected adults (2002-2008)
Abstract
Objective: Prior research has documented sociodemographic disparities in the use of antiretroviral therapy (ART). Recent therapeutic developments and changing epidemiological profiles may have altered such disparities. We examine the extent to which sociodemographic differences in prescribed ART have changed between 2002 and 2008.
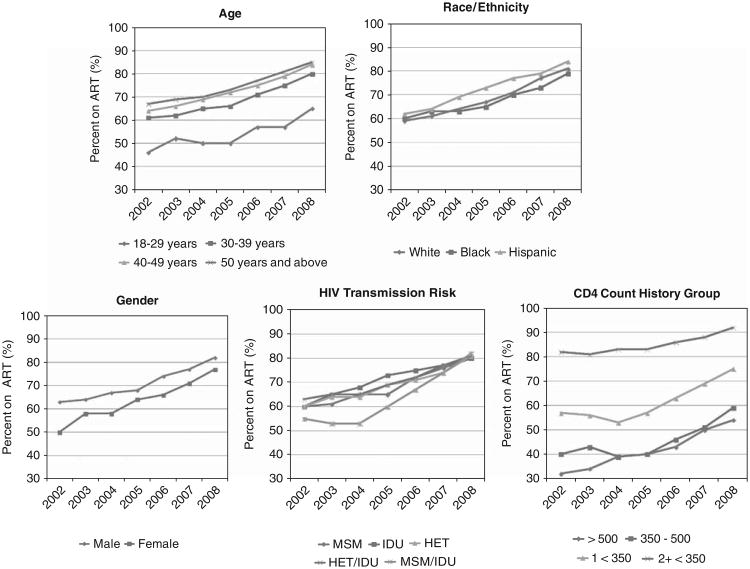
Methods: We analyzed data abstracted from medical records at 13 US sites participating in the Human Immunodeficiency Virus Research Network. Prescription of ART was assessed for each year in care for each patient. A total of 14,092 patients were followed up for 39,251 person-years. We examined ART use as a function of sex, race/ethnicity, human immunodeficiency virus risk group, age, and CD4 history (no test <500 cells/mm, one or more tests between 500 and 350 cells/mm, 1 test ≤350 cells/mm, and 2 or more tests ≤350 cells/mm). Using multiple logistic regression, we ascertained interactions between each of these variables and calendar year.
Results: The overall percentage prescribed ART increased from 60% to 80% between 2002 and 2008. Among those with 2 or more CD4 tests ≤350 cells/mm, the percentage increased from 82% to 92%. ART rates were higher for those with lower CD4 counts but increased over time for all CD4 groups and for all demographic groups. Nevertheless, sex and racial/ethnic disparities persisted. Significant interactions were obtained for CD4 history by year, age by year, and age by CD4 history.
Conclusions: Although prescription of ART became more widespread from 2002 to 2008, patients who were female, black, or younger still had lower ART rates than male, white, or older patients.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Ledergerber B, Egger M, Erard V, et al. AIDS-related opportunistic illnesses occurring after initiation of potent antiretroviral therapy: the Swiss HIV Cohort Study. JAMA. 1999;282:2220–2226. - PubMed
-
- Moore RD, Chaisson RE. Natural history of HIV infection in the era of combination antiretroviral therapy. AIDS. 1999;13:1933–1942. - PubMed
-
- Palella FJ, Jr, Delaney KM, Moorman AC, et al. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. HIV Outpatient Study Investigators. N Engl J Med. 1998;338:853–860. - PubMed
-
- Gebo KA, Diener-West M, Moore RD. Hospitalization rates in an urban cohort after the introduction of highly active antiretroviral therapy. J Acquir Immune Defic Syndr. 2001;27:143–152. - PubMed
-
- Torres RA, Barr M. Impact of combination therapy for HIV infection on inpatient census. N Engl J Med. 1997;336:1531–1532. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
