

Costs and trends in pancreatic cancer treatment
- PMID: 22415469
- PMCID: PMC5018231
- DOI: 10.1002/cncr.27490
Costs and trends in pancreatic cancer treatment
Abstract
Background: Pancreatic cancer poses a substantial morbidity and mortality burden in the United States, and predominantly affects older adults. The objective of this study was to estimate the direct medical costs of pancreatic cancer treatment in a population-based cohort of Medicare beneficiaries, and the contribution of different treatment modalities and health care services to the total cost of care and trends in costs over time.
Methods: In the linked Surveillance, Epidemiology, and End Results (SEER)-Medicare database, pancreatic cancer patients were identified who were aged 66 years or older and who were diagnosed from 2000 to 2007. Total direct medical costs were estimated from Medicare payments overall and within categories of care. Costs attributable to pancreatic cancer were estimated by subtracting the costs of medical care in a matched cohort of cancer-free beneficiaries.
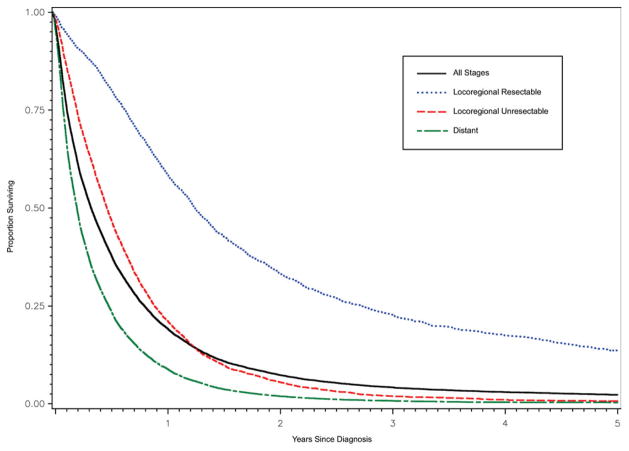
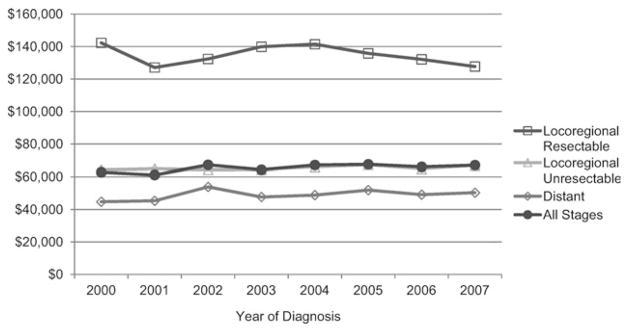
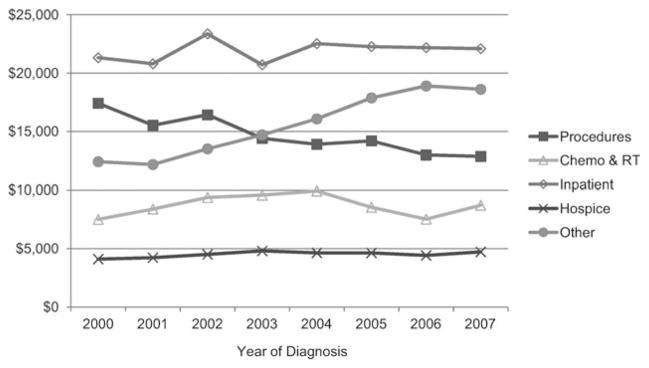
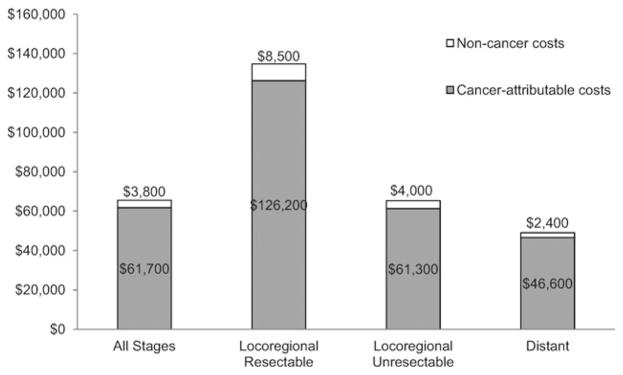
Results: A total of 15,037 patients were identified, of whom 97% were observed from diagnosis until death. Mean total direct medical costs were $65,500. Mean total costs were greater for patients with resectable locoregional disease ($134,700) than for those with unresectable locoregional or distant disease ($65,300 and $49,000, respectively). Hospitalizations and cancer-directed procedures collectively accounted for the largest fraction of health care costs. The total cost of care appeared to increase slightly over the study period (P = .05). The mean costs attributable to pancreatic cancer were $61,700.
Conclusions: Despite poor prognosis and short survival, the economic burden of pancreatic cancer in the elderly is substantial. Demographic trends, greater use of targeted therapies, and possible implementation of screening strategies are likely to impact treatment patterns and costs in the future.
Copyright © 2012 American Cancer Society.
Conflict of interest statement
DISCLOSURE Ms. O’Neill is supported by the Health Research Board (Ireland) through the HRB PhD Scholars Programme in Health Service Research (grant PHD/2007/16). Dr. Elkin is supported by a Career Development Award from the National Cancer Institute (grant 1K07CA118189).
Figures
References
-
- Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA Cancer J Clin. 2010;60:277–300. - PubMed
-
- American Cancer Society. [Accessed Oct 1, 2011];Cancer Facts &; Figures. 2010 http://www.cancer.org/Research/CancerFactsFigures/CancerFactsFigures/can....
-
- Stathis A, Moore MJ. Advanced pancreatic carcinoma: current treatment and future challenges. Nat Rev Clin Oncol. 2010;7:163–172. - PubMed
-
- Chua YJ, Zalcberg JR. Pancreatic cancer–is the wall crumbling? Ann Oncol. 2008;19:1224–1230. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
