

Association of hospital spending intensity with mortality and readmission rates in Ontario hospitals
- PMID: 22416099
- PMCID: PMC3339410
- DOI: 10.1001/jama.2012.265
Association of hospital spending intensity with mortality and readmission rates in Ontario hospitals
Abstract
Context: The extent to which better spending produces higher-quality care and better patient outcomes in a universal health care system with selective access to medical technology is unknown.
Objective: To assess whether acute care patients admitted to higher-spending hospitals have lower mortality and readmissions.
Design, setting, and patients: The study population comprised adults (>18 years) in Ontario, Canada, with a first admission for acute myocardial infarction (AMI) (n = 179,139), congestive heart failure (CHF) (n = 92,377), hip fracture (n = 90,046), or colon cancer (n = 26,195) during 1998-2008, with follow-up to 1 year. The exposure measure was the index hospital's end-of-life expenditure index for hospital, physician, and emergency department services.
Main outcome measures: The primary outcomes were 30-day and 1-year mortality and readmissions and major cardiac events (readmissions for AMI, angina, CHF, or death) for AMI and CHF.
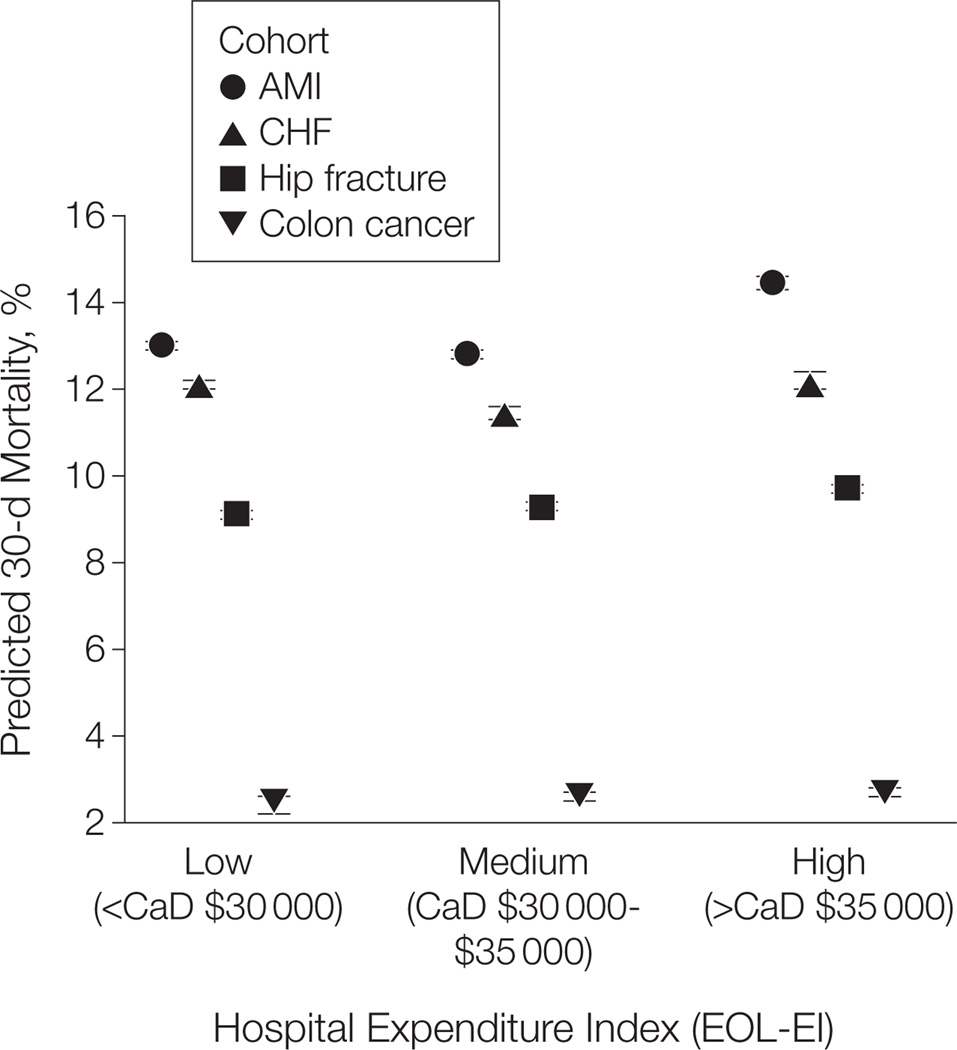
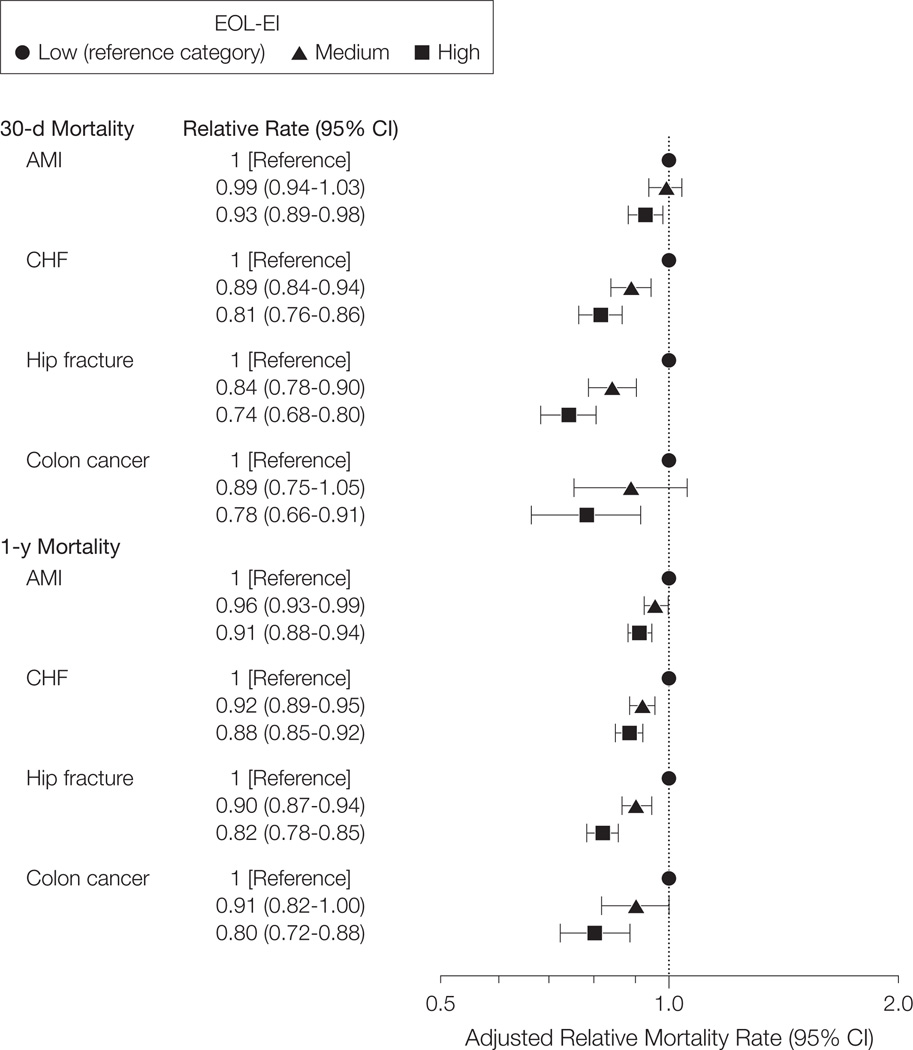
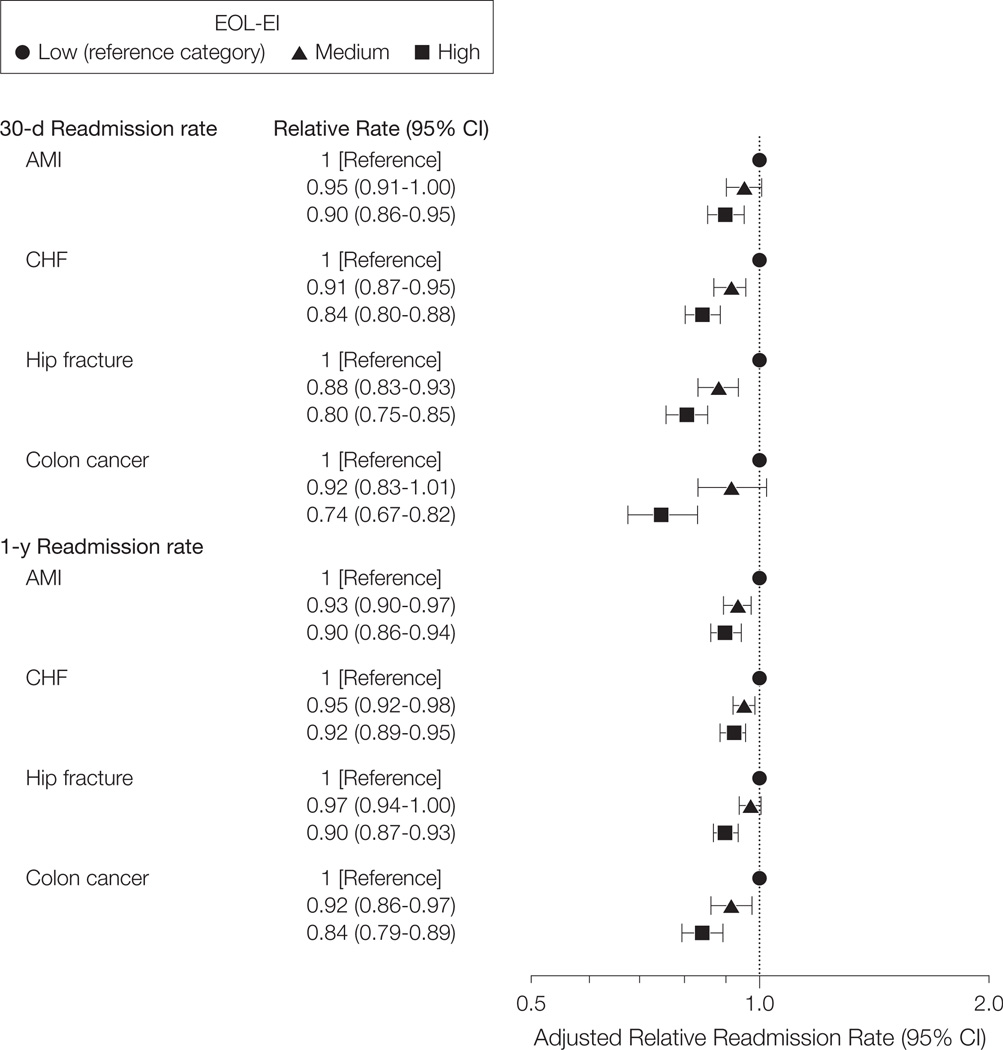
Results: Patients' baseline health status was similar across hospital expenditure groups. Patients admitted to hospitals in the highest- vs lowest-spending intensity terciles had lower rates of all adverse outcomes. In the highest- vs lowest-spending hospitals, respectively, the age- and sex-adjusted 30-day mortality rate was 12.7% vs 12.8% for AMI, 10.2% vs 12.4% for CHF, 7.7% vs 9.7% for hip fracture, and 3.3% vs 3.9% for CHF; fully adjusted relative 30-day mortality rates were 0.93 (95% CI, 0.89-0.98) for AMI, 0.81 (95% CI, 0.76-0.86) for CHF, 0.74 (95% CI, 0.68-0.80) for hip fracture, and 0.78 (95% CI, 0.66-0.91) for colon cancer. Results for 1-year mortality, readmissions, and major cardiac events were similar. Higher-spending hospitals had higher nursing staff ratios, and their patients received more inpatient medical specialist visits, interventional (AMI cohort) and medical (AMI and CHF cohorts) cardiac therapies, preoperative specialty care (colon cancer cohort), and postdischarge collaborative care with a cardiologist and primary care physician (AMI and CHF cohorts).
Conclusion: Among Ontario hospitals, higher spending intensity was associated with lower mortality, readmissions, and cardiac event rates.
Conflict of interest statement
Figures
Comment in
-
The relationship between cost and quality: no free lunch.JAMA. 2012 Mar 14;307(10):1082-3. doi: 10.1001/jama.2012.287. JAMA. 2012. PMID: 22416105 No abstract available.
Similar articles
-
Association of Early Physician Follow-up With Readmission Among Patients Hospitalized for Acute Myocardial Infarction, Congestive Heart Failure, or Chronic Obstructive Pulmonary Disease.JAMA Netw Open. 2022 Jul 1;5(7):e2222056. doi: 10.1001/jamanetworkopen.2022.22056. JAMA Netw Open. 2022. PMID: 35819782 Free PMC article.
-
Association between hospital cardiac management and outcomes for acute myocardial infarction patients.Med Care. 2010 Feb;48(2):157-65. doi: 10.1097/MLR.0b013e3181bd4da7. Med Care. 2010. PMID: 19927014
-
Impact on hospital ranking of basing readmission measures on a composite endpoint of death or readmission versus readmissions alone.BMC Health Serv Res. 2017 May 5;17(1):327. doi: 10.1186/s12913-017-2266-4. BMC Health Serv Res. 2017. PMID: 28476128 Free PMC article.
-
Clinical Outcomes of Acute Myocardial Infarction Hospitalizations With Systemic Lupus Erythematosus: An Analysis of Nationwide Readmissions Database.Curr Probl Cardiol. 2022 Nov;47(11):101086. doi: 10.1016/j.cpcardiol.2021.101086. Epub 2021 Dec 20. Curr Probl Cardiol. 2022. PMID: 34936910 Review.
-
Does Higher Spending Improve Survival Outcomes for Myocardial Infarction? Examining the Cost-Outcomes Relationship Using Time-Varying Covariates.Health Serv Res. 2015 Oct;50(5):1589-605. doi: 10.1111/1475-6773.12286. Epub 2015 Feb 9. Health Serv Res. 2015. PMID: 25664611 Free PMC article. Review.
Cited by
-
High resource utilization does not affect mortality in acute respiratory failure patients managed with tracheostomy.Respir Care. 2013 Nov;58(11):1863-72. doi: 10.4187/respcare.02359. Epub 2013 Apr 30. Respir Care. 2013. PMID: 23650434 Free PMC article.
-
Regional variation in healthcare spending and mortality among senior high-cost healthcare users in Ontario, Canada: a retrospective matched cohort study.BMC Geriatr. 2018 Nov 1;18(1):262. doi: 10.1186/s12877-018-0952-7. BMC Geriatr. 2018. PMID: 30382828 Free PMC article.
-
Cardiac intervention rates for older patients with acute myocardial infarction in the United States and Ontario, 2003-2013: a retrospective cohort study.CMAJ Open. 2020 Jun 11;8(2):E437-E447. doi: 10.9778/cmajo.20190190. Print 2020 Apr-Jun. CMAJ Open. 2020. PMID: 32527795 Free PMC article.
-
Impact of Physician-Coordinated Intensive Follow-Up on Long-Term Medical Costs in Patients with Unstable Angina Undergoing Percutaneous Coronary Intervention.Acta Cardiol Sin. 2017 Mar;33(2):173-181. doi: 10.6515/acs20160521a. Acta Cardiol Sin. 2017. PMID: 28344421 Free PMC article.
-
End-of-Life Care Interventions: An Economic Analysis.Ont Health Technol Assess Ser. 2014 Dec 1;14(18):1-70. eCollection 2014. Ont Health Technol Assess Ser. 2014. PMID: 26339303 Free PMC article. Review.
References
-
- Fisher ES, Wennberg DE, Stukel TA, Gottlieb DJ, Lucas FL, Pinder EL. The implications of regional variations in Medicare spending, 1: the content, quality, and accessibility of care. Ann Intern Med. 2003;138(4):273–287. - PubMed
-
- Fisher ES, Wennberg DE, Stukel TA, Gottlieb DJ, Lucas FL, Pinder EL. The implications of regional variations in Medicare spending-2: health outcomes and satisfaction with care. Ann Intern Med. 2003;138(4):288–298. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
