

Proton beam therapy and concurrent chemotherapy for esophageal cancer
- PMID: 22417808
- PMCID: PMC3923631
- DOI: 10.1016/j.ijrobp.2012.01.003
Proton beam therapy and concurrent chemotherapy for esophageal cancer
Abstract
Purpose: Proton beam therapy (PBT) is a promising modality for the management of thoracic malignancies. We report our preliminary experience of treating esophageal cancer patients with concurrent chemotherapy (CChT) and PBT (CChT/PBT) at MD Anderson Cancer Center.
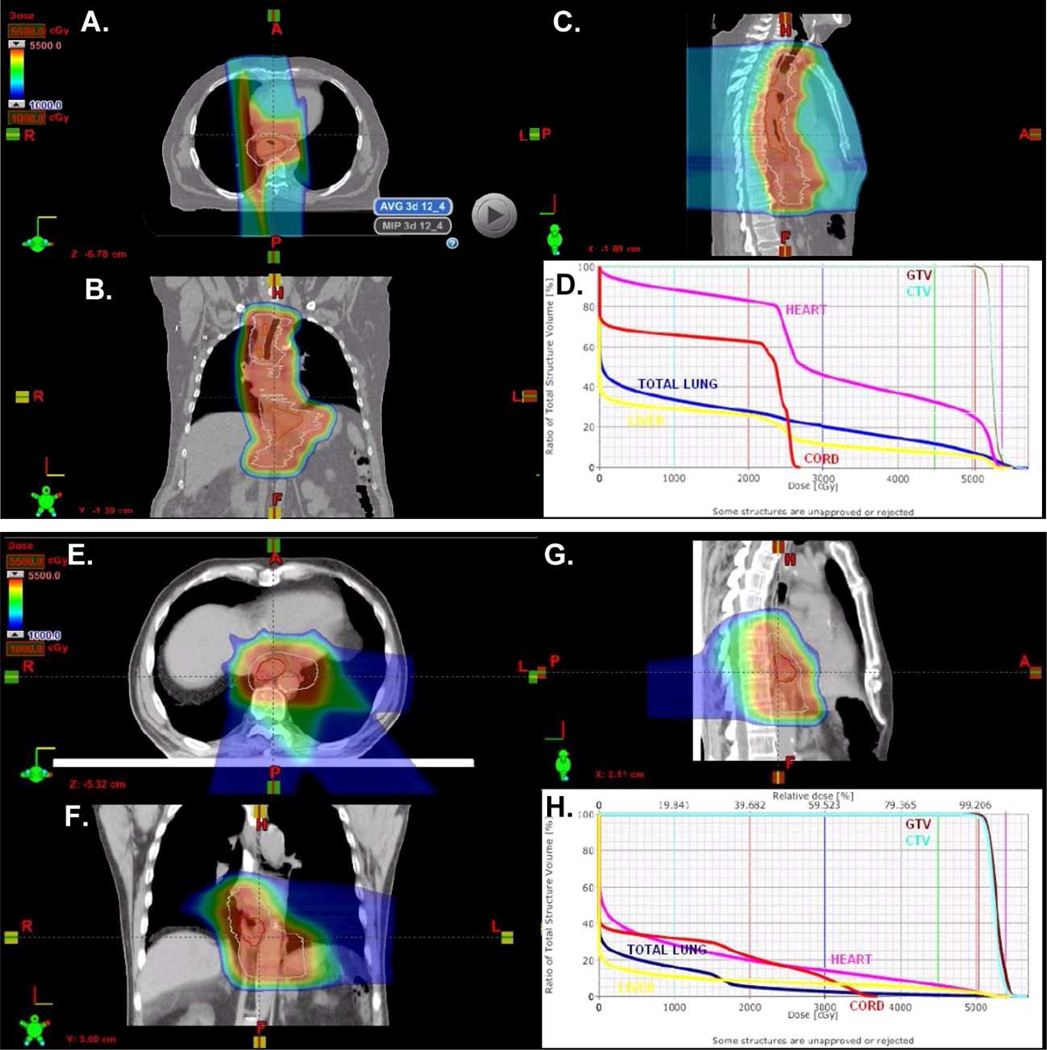
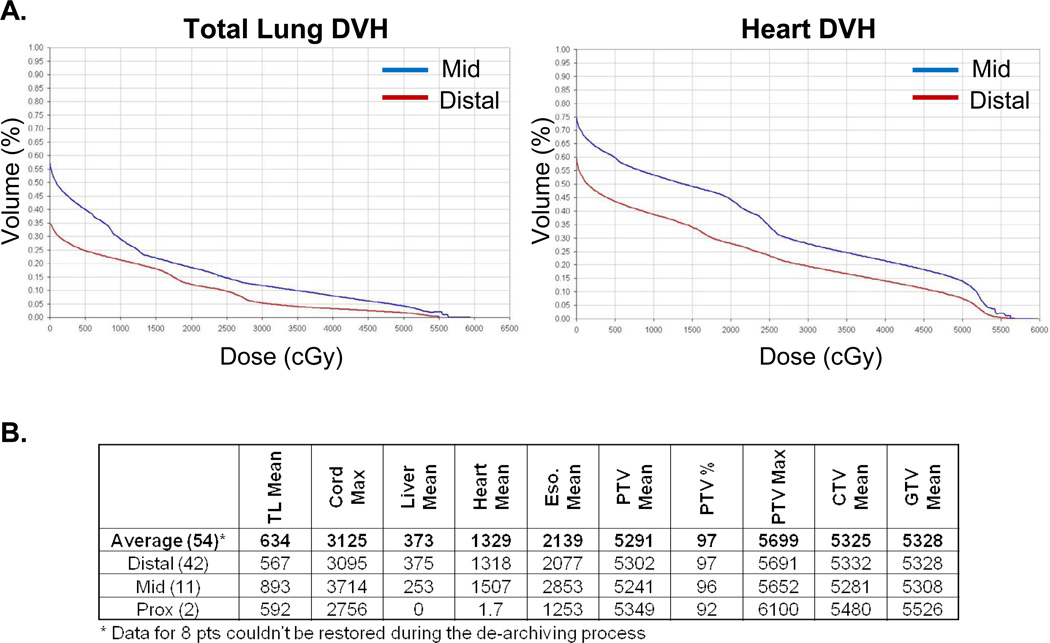
Methods and materials: This is an analysis of 62 esophageal cancer patients enrolled on a prospective study evaluating normal tissue toxicity from CChT/PBT from 2006 to 2010. Patients were treated with passive scattering PBT with two- or three-field beam arrangement using 180 to 250 MV protons. We used the Kaplan-Meier method to assess time-to-event outcomes and compared the distributions between groups using the log-rank test.
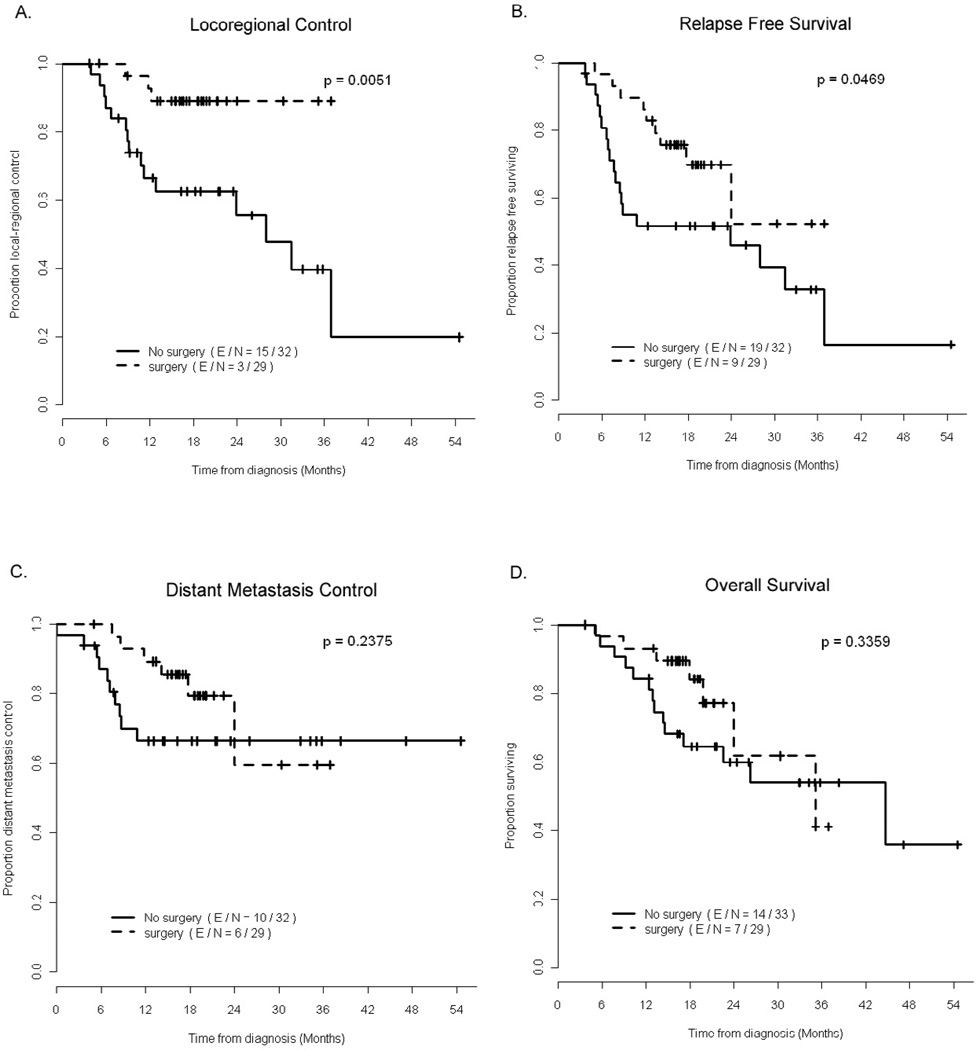
Results: The median follow-up time was 20.1 months for survivors. The median age was 68 years (range, 38-86). Most patients were males (82%) who had adenocarcinomas (76%) and Stage II-III disease (84%). The median radiation dose was 50.4 Gy (RBE [relative biologic equivalence]) (range, 36-57.6). The most common grade 2 to 3 acute toxicities from CChT/PBT were esophagitis (46.8%), fatigue (43.6%), nausea (33.9%), anorexia (30.1%), and radiation dermatitis (16.1%). There were two cases of grade 2 and 3 radiation pneumonitis and two cases of grade 5 toxicities. A total of 29 patients (46.8%) received preoperative CChT/PBT, with one postoperative death. The pathologic complete response (pCR) rate for the surgical cohort was 28%, and the pCR and near CR rates (0%-1% residual cells) were 50%. While there were significantly fewer local-regional recurrences in the preoperative group (3/29) than in the definitive CChT/PBT group (16/33) (log-rank test, p = 0.005), there were no differences in distant metastatic (DM)-free interval or overall survival (OS) between the two groups.
Conclusions: This is the first report of patients treated with PBT/CChT for esophageal cancer. Our data suggest that this modality is associated with a few severe toxicities, but the pathologic response and clinical outcomes are encouraging. Prospective comparison with more traditional approach is warranted.
Copyright © 2012 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Jemal A, Siegel R, Xu J, et al. Cancer statistics, 2010. CA Cancer Journal for Clinicians. 60:277–300. - PubMed
-
- Ruderman AI, Kondratyeva AP, Ratner TG. Proton beam irradiation in esophageal cancer. Meditsinskaya Radiologiya. 1981;26:20–25. - PubMed
-
- Isacsson U, Lennernäs B, Grusell E, et al. Comparative treatment planning between proton and x-ray therapy in esophageal cancer. International Journal of Radiation Oncology Biology Physics. 1998;41:441–450. - PubMed
-
- Sugahara S, Tokuuye K, Okumura T, et al. Clinical results of proton beam therapy for cancer of the esophagus. International Journal of Radiation Oncology Biology Physics. 2005;61:76–84. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
