

Local pulmonary administration of factor VIIa (rFVIIa) in diffuse alveolar hemorrhage (DAH) - a review of a new treatment paradigm
- PMID: 22419859
- PMCID: PMC3299534
- DOI: 10.2147/BTT.S25507
Local pulmonary administration of factor VIIa (rFVIIa) in diffuse alveolar hemorrhage (DAH) - a review of a new treatment paradigm
Abstract
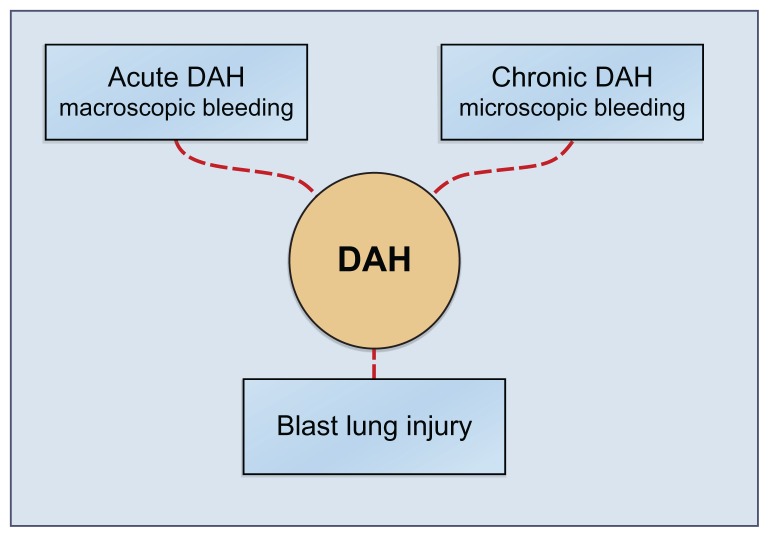
Background: Diffuse alveolar hemorrhage (DAH) is a clinical syndrome with typical symptoms dyspnea and hemoptysis. DAH is a complication of specific diseases, in some cases with acute catastrophic hemoptysis, while other patients present low grade alveolar bleeding with a need of chronic transfusion as in pulmonary hemosiderosis.
Methods: Current literature in the PubMed database and other sources was reviewed in order to evaluate the current treatment recommendations, efficacy of this treatment, and finally the risk of complications after off-label use of rFVIIa in respect to DAH.
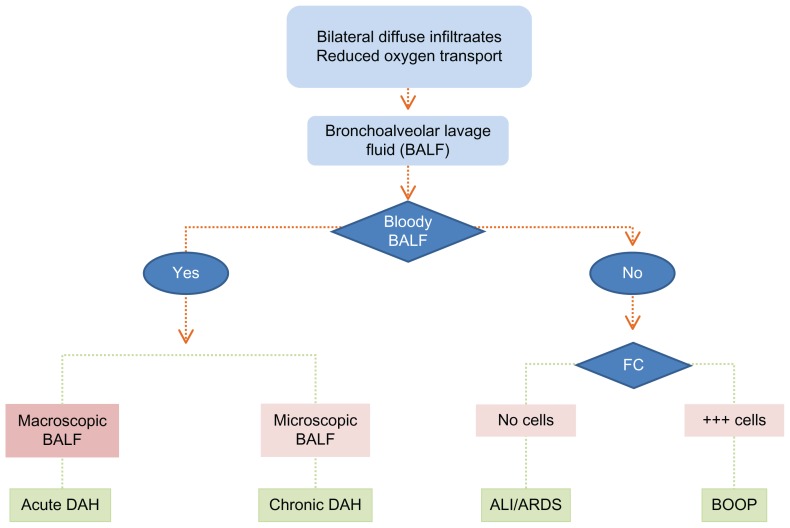
Objectives: (i) To elucidate the clinical aspects of alveolar hemorrhage, (ii) to develop a simple diagnostic algorithm in order to separate DAH from other important pulmonary diseases with similar clinical picture and comparably high mortality. Such an algorithm has important therapeutic consequences because these diseases: acute lung injury (ALI), acute respiratory distress syndrome (ARDS) and bronchiolitis obliterans organizing pneumonia (BOOP) have different therapies, (iii) to evaluate and discuss whether local pulmonary administration may improve outcome and reduce mortality in DAH, and (iv) to suggest a treatment schedule.
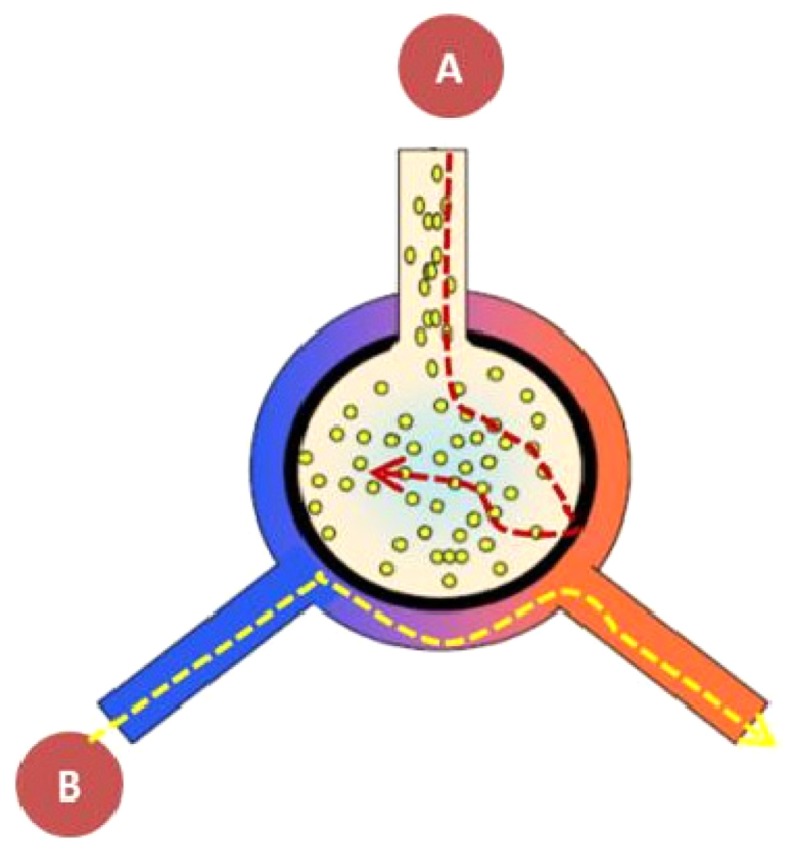
Results: Hitherto the diagnosis and treatment of DAH has been based on anecdotal reports. The treatment has relied on different unspecific treatment modalities based on a mixture of treatment of the underlying disease and treatment without evidence targeted to stop the alveolar bleeding. However, recently a number of publications have advocated the use of intrapulmonary rFVIIa. Even in severe bleeding DAH has been shown to respond promptly without thromboembolic complication when FVIIa was administered locally via the air side, because the FVIIa does not penetrate the alveolo-capillary membrane to the blood-side. The incidence of DAH (in the US and Europe is 100,000-150,000, and 50,000 patients annually are at risk of developing DAH following hematopoietic stem cell transplant (HSCT) and autoimmune diseases. Finally 50,000-100,000 patients may be falsely categorized as having acute respiratory distress syndrome/acute lung injury (ARDS/ALI) because DAH and ARDS cannot be separated clinically. A new treatment paradigm of DAH is proposed as no other intervention has been able to ensure pulmonary hemostasis in DAH. The diagnosis of DAH is simple, a series of broncho-alveolar washes which become increasingly bloody. This test should be performed in all patients with pulmonary opacities in order to separate ARDS/ALI from DAH. FVIIa administrated via pulmonary route is "drug of choice", because it stops bleeding in the life-threatening syndrome DAH. Hemostasis is obtained after only one to two small doses of FVIIa (50 μg/kg body weight per dose) and after hemostasis the oxygen transport quickly improves.
Conclusion: Intrapulmonary administration of rFVIIa is recommended as the treatment of choice for DAH and blast lung injury (BLI) because the treatment has been shown to be successful and uncomplicated in spite of the fact that only a small series of DAH has been documented.
Keywords: algorithm; biologics; blast lung injury; bronchoalveolar lavage; coagulation factor FVIIa; diagnosis; diffuse alveolar hemorrhage; hemosiderosis; local pulmonary treatment; new treatment recommendation.
Figures


References
-
- Rose RM, Kobzik L, Dushay K, et al. The effect of aerosolized recombinant human granulocyte macrophage colony-stimulating factor on lung leukocytes in nonhuman primates. Am Rev Respir Dis. 1992;146(5 Pt 1):1279–1286. - PubMed
-
- Choi G, Vlaar APJ, Schouten M, et al. Natural anticoagulants limit lipopolysaccharide-induced pulmonary coagulation but not inflammation. Eur Respir J. 2007;30(3):423–428. - PubMed
-
- Heslet L. Look on the “air side” in pneumonia. Crit Care Med. 2009;37(2):774–775. - PubMed
-
- Afessa B, Tefferi A, Litzow MR, et al. Diffuse alveolar hemorrhage in hematopoietic stem cell transplant recipients. Am J Respir Crit Care Med. 2002;166(5):64–645. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
