

Stimulant medication use in children: a 12-year perspective
- PMID: 22420039
- PMCID: PMC3548321
- DOI: 10.1176/appi.ajp.2011.11030387
Stimulant medication use in children: a 12-year perspective
Abstract
Objective: The authors examined the utilization of stimulant medications for the treatment of ADHD in U.S. children during the period 1996–2008 to determine trends by age, sex, race/ethnicity, family income, and geographic region.
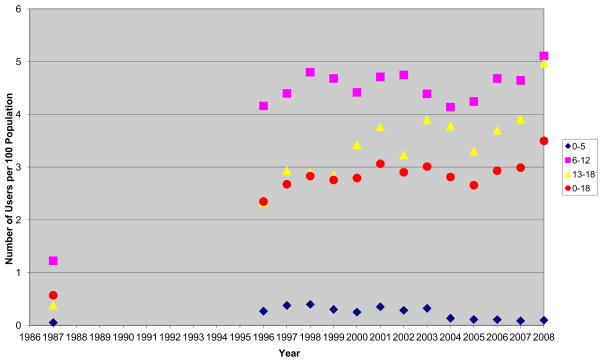
Method: The 1996–2008 database of the Medical Expenditure Panel Survey, a nationally representative annual survey of U.S. households, was analyzed for therapeutic stimulant use in children age 18 and younger. The data for 1987 were also recalculated for reference.
Results: An estimated 3.5% (95% confidence interval=3.0–4.1) of U.S. children received stimulant medication in 2008, up from 2.4% in 1996. Over the period 1996–2008, stimulant use increased consistently at an overall annual growth rate of 3.4%. Use increased in adolescents (annual growth, 6.5%), but it did not significantly change in 6- to 12-year-olds, and it decreased in preschoolers. Use remained higher in boys than in girls, and it remained consistently lower in the West than in other U.S. regions. While differences by family income have disappeared over time, use of stimulants in ADHD treatment is significantly lower in racial/ethnic minorities.
Conclusions: Overall, pediatric stimulant use has been slowly but steadily increasing since 1996, primarily as a result of greater use in adolescents. Use in preschoolers remains low and has declined over time. Important variations related to racial/ethnic background and geographic region persist, thus indicating a substantial heterogeneity in the approach to the treatment of ADHD in U.S. communities.
Conflict of interest statement
Disclaimer/Disclosure: The opinions and assertions contained in this report are the private views of the authors and are not to be construed as official or as reflecting the views of the Agency for Healthcare Research and Quality, the National Institute of Mental Health, or the U.S. Department of Health and Human Services. The authors report no relevant conflicts of interest.
Figures
Comment in
-
ADHD pharmacotherapy: rates of stimulant use and cardiovascular risk.Am J Psychiatry. 2012 Feb;169(2):112-4. doi: 10.1176/appi.ajp.2011.11111703. Am J Psychiatry. 2012. PMID: 22318789 No abstract available.
References
-
- Zito JM, Safer DJ, DosReis S, Gardner JF, Magder L, Soeken K, Boles M, Lynch F, Riddle MA. Psychotropic practice patterns for youth: a 10-year perspective. Arch Pediatr Adolesc Med. 2003;157(1):17–25. - PubMed
-
- Pliszka S AACAP Workgroup on Quality Issues. Practice Parameter for the Assessment and Treatment of Children and Adolescents With Attention-Deficit/Hyperactivity Disorder. J Am Acad Child Adolesc Psychiatry. 2007;46(7):894–921. - PubMed
-
- Olfson M, Gameroff MJ, Marcus SC, Jensen PS. National trends in the treatment of attention deficit hyperactivity disorder. Am J Psychiatry. 2003 Jun;160(6):1071–7. - PubMed
-
- Zuvekas SH, Vitiello B, Norquist NS. Recent trends in stimulant medication use among U.S. children. Am J Psychiatry. 2006;163:579–585. - PubMed
-
- Scheffler RM, Hinshaw SP, Modrek S, Levine P. The global market for ADHD medications. Health Affairs. 2007;26:450–457. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
