

Knowledge of quality performance measures associated with endoscopy among gastroenterology trainees and the impact of a web-based intervention
- PMID: 22421498
- PMCID: PMC3739290
- DOI: 10.1016/j.gie.2012.01.019
Knowledge of quality performance measures associated with endoscopy among gastroenterology trainees and the impact of a web-based intervention
Abstract
Background: Knowledge of quality measures in endoscopy among trainees is unknown.
Objective: To assess knowledge of endoscopy-related quality indicators among U.S. trainees and determine whether it improves with a Web-based intervention.
Design: Randomized, controlled study.
Setting: Multicenter.
Participants: This study involved trainees identified from the American Society for Gastrointestinal Endoscopy membership database.
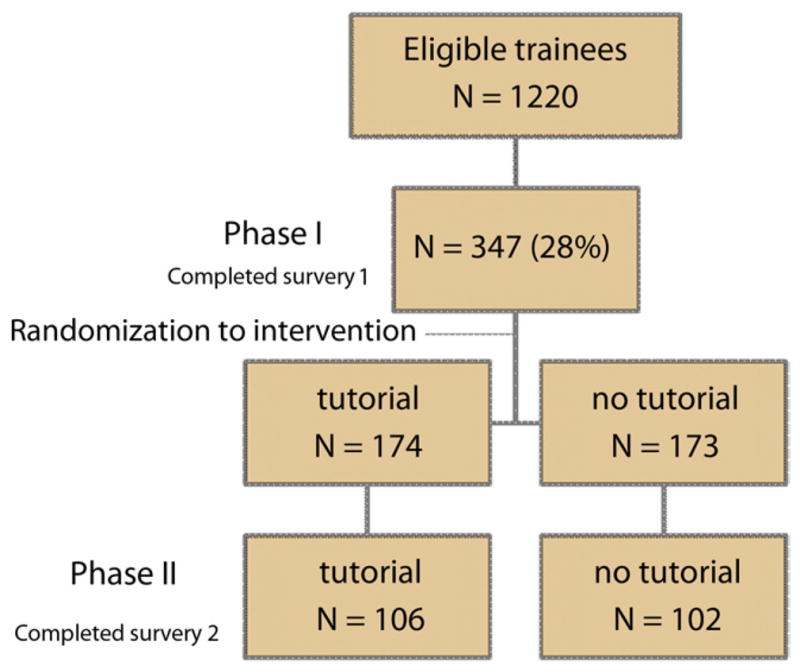
Intervention: Participants were invited to complete an 18-question online test. Respondents were randomized to receive a Web-based tutorial (intervention) or not. The test was readministered 6 weeks after randomization to determine the intervention's impact.
Main outcome measurements: Baseline knowledge of endoscopy-related quality indicators and impact of the tutorial.
Results: A total of 347 of 1220 trainees (28%) completed the test; the mean percentage of correct responses was 55%. For screening colonoscopy, 44% knew the adenoma detection rate benchmark, 42% identified the cecal intubation rate goal, and 74% knew the recommended minimum withdrawal time. A total of 208 of 347 trainees (59%) completed the second test; baseline scores were similar for the tutorial (n = 106) and no tutorial (n = 102) groups (56.4% vs 56.9%, respectively). Scores improved after intervention for the tutorial group (65%, P = .003) but remained unchanged in the no tutorial group. On multivariate analysis, each additional year in training (odds ratio [OR] 2.3; 95% confidence interval [CI], 1.5-3.4), training at an academic institution (OR 2.6; 95% CI, 1.1-6.3), and receiving the tutorial (OR 3.2; 95% CI, 1.7-5.9) were associated with scores in the upper tertile.
Limitations: Low response rate.
Conclusion: Knowledge of endoscopy-related quality performance measures is low among trainees but can improve with a Web-based tutorial. Gastroenterology training programs may need to incorporate a formal didactic curriculum to supplement practice-based learning of quality standards in endoscopy.
Copyright © 2012 American Society for Gastrointestinal Endoscopy. Published by Mosby, Inc. All rights reserved.
Comment in
-
Getting the word out about quality measures.Gastrointest Endosc. 2012 Jul;76(1):107-9. doi: 10.1016/j.gie.2012.02.057. Gastrointest Endosc. 2012. PMID: 22726469 No abstract available.
References
-
- Rex DK, Petrini JL, Baron TH, et al. ASGE/ACG Taskforce on Quality in Endoscopy. Quality indicators for colonoscopy. Am J Gastroenterol. 2006;101:886–91. - PubMed
-
- AGA Task Force on Quality in Practice: A national overview and implications for GI practice. Gastroenterology. 2005;129:361–9. - PubMed
-
- Petersen BT. Demand the Data! Your patients will ask and your practice will need it. Am J Gastroenterol. 2007;102:862–3. - PubMed
-
- Cotton PB, Hawes RH, Barkun A, et al. Excellence in endoscopy: toward practical metrics. Gastrointest Endosc. 2006;63:286–91. - PubMed
-
- American Society for Gastrointestinal Endoscopy. Quality and outcomes assessment in gastrointestinal endoscopy. Gastrointest Endosc. 2000;52:827–30. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
