

Case Reports
doi: 10.3174/ajnr.A2964.
Epub 2012 Mar 15.
Multimodal imaging of reversible cerebral vasoconstriction syndrome: a series of 6 cases
Affiliations
- PMID: 22422190
- PMCID: PMC7965494
- DOI: 10.3174/ajnr.A2964
Item in Clipboard
Case Reports
Multimodal imaging of reversible cerebral vasoconstriction syndrome: a series of 6 cases
AJNR Am J Neuroradiol.
2012 Aug.
Abstract
RCVS is a clinical condition of recurrent severe headaches that may be associated with ischemic or hemorrhagic stroke and that is defined by the presence of segmental vasoconstriction in multiple cerebral arteries. The angiographic appearance resembles vasculitis, except that the abnormalities resolve during the course of several months. Because the treatment of RCVS differs from that for vasculitis, radiologists must understand the clinical and radiologic features so as to better guide imaging algorithms and facilitate diagnosis. We present a series of 6 cases of RCVS that highlight the imaging features across multiple modalities.
Figures
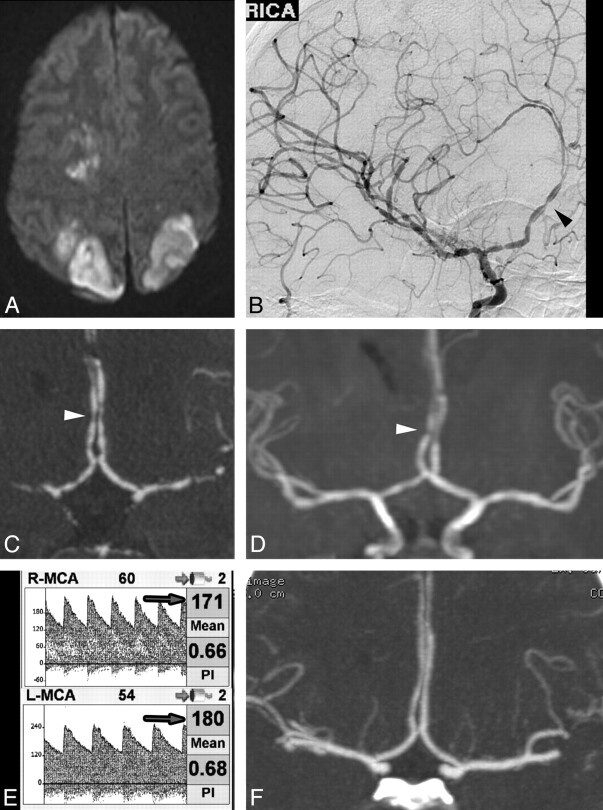
A, MR imaging DWI sequence demonstrates acute infarctions in several vascular territories. Angiography (DSA, CTA, and MRA) performed at the same time reveals widespread areas of severe vascular narrowing alternating with vasodilation (arrowheads). B, DSA, right ICA transorbital oblique projection. C, CTA, coronal MIP reformat. D, MRA, coronal MIP reformat. E, TCD demonstrates elevated MCA flow velocities bilaterally (arrows). F, Coronal MIP reformat of CTA performed 11 months later demonstrates normalization of vessel caliber and contour.
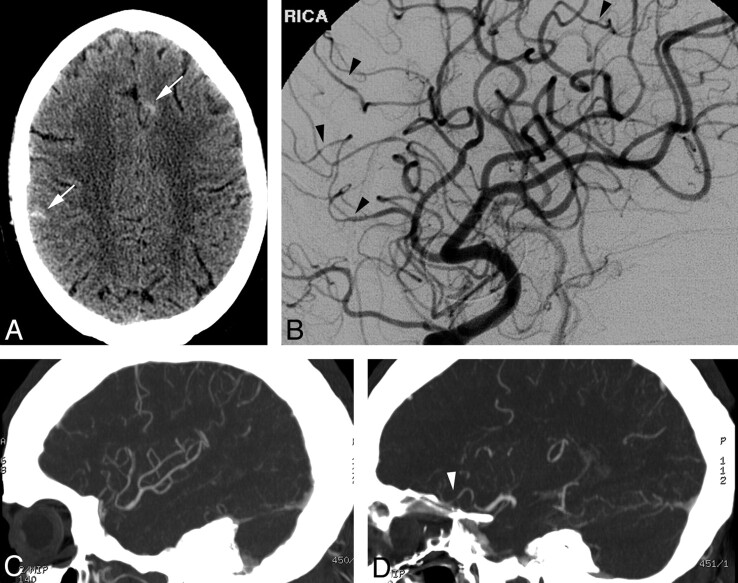
A, NCCT demonstrates scattered sulcal SAH (arrows). B, DSA, right ICA oblique lateral projection, demonstrates subtle areas of vessel narrowing and dilation in several small-caliber arteries. C and D, MIP reformats from CTA performed the same day demonstrate normal large and medium right MCA branches (C) but do not convincingly demonstrate the abnormal small-caliber arteries (arrowhead, D), illustrating the limitations of CTA.
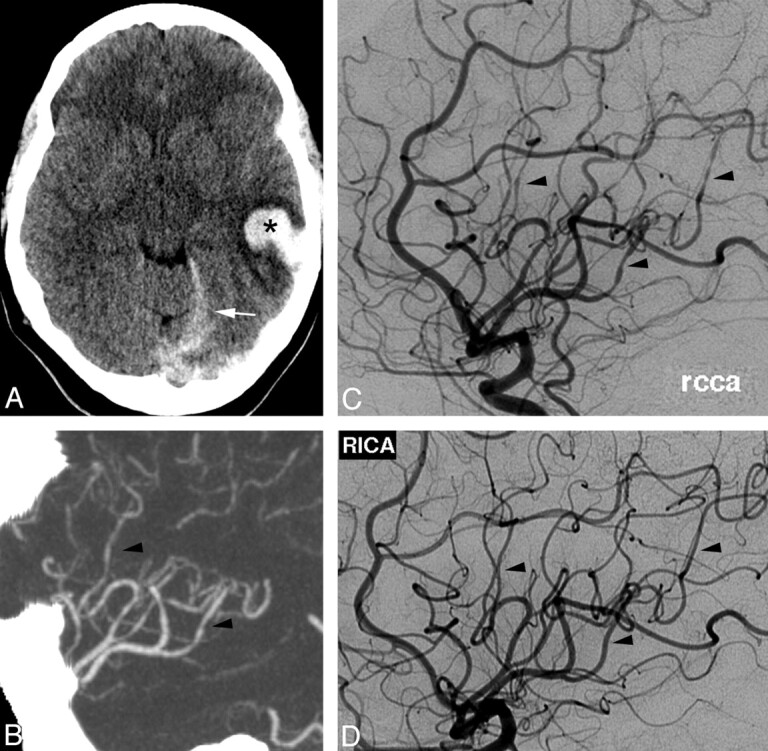
A, NCCT demonstrates left temporal IPH (asterisk) and tentorial SDH (arrow). B, CTA MIP reformat, demonstrates subtle irregularity of the distal right MCA branches (not prospectively recognized). C, DSA, right common carotid artery, Haughton projection, shows multiple areas of vascular narrowing of medium- and small-caliber vessels (arrowheads). D, Findings resolved on follow-up DSA, right ICA Haughton projection, 2 months later.
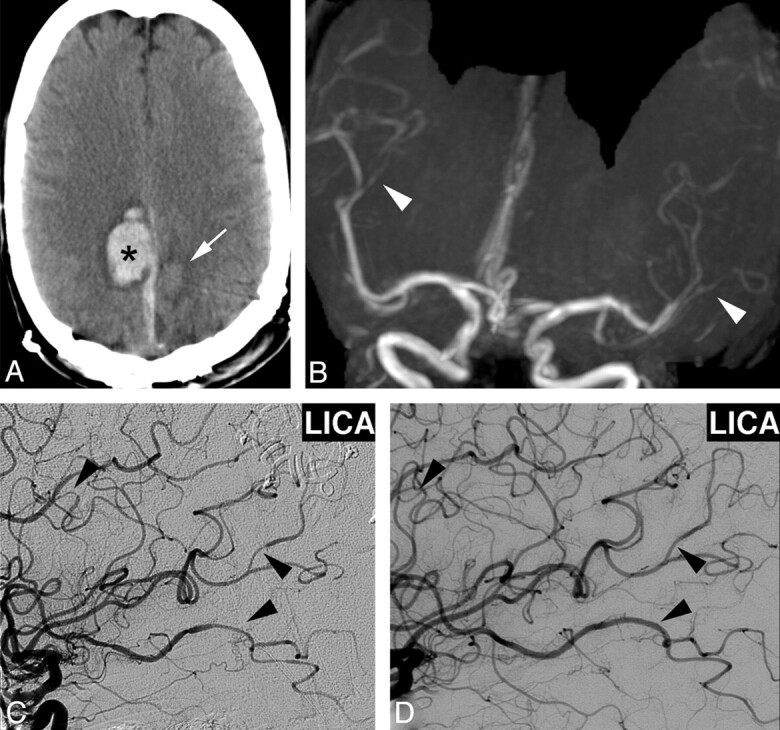
A, NCCT 1 week after initial presentation demonstrates right posterior frontal IPH (asterisk), right parafalcine SDH, and subacute left posterior frontal IPH (arrow). B and C, MRA coronal MIP reformat shows irregular narrowing of distal MCA branches (white arrowheads, B), which was confirmed on DSA, left ICA injection (arrowheads, C). D, Repeat DSA 3 months later demonstrates resolution of vascular findings.
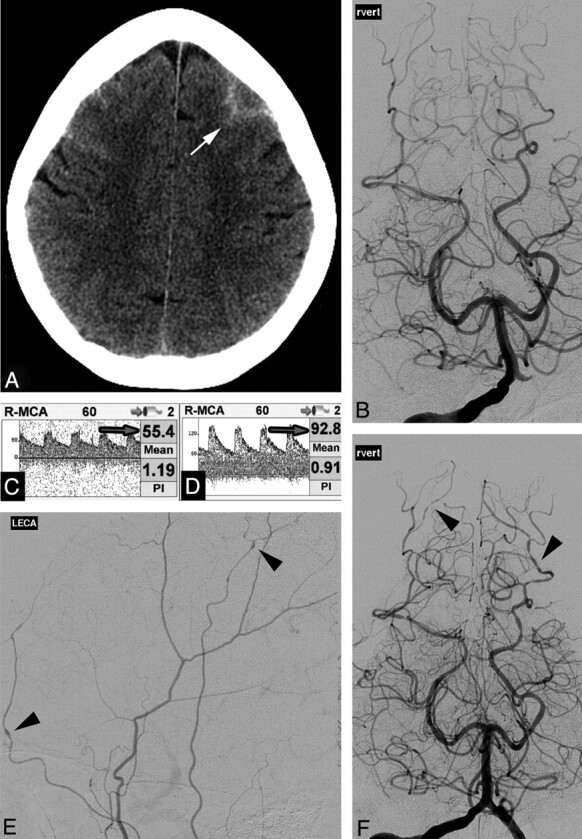
A, NCCT demonstrates frontal convexal SAH (arrow). B, DSA findings, right vertebral injection, are normal on presentation. C and D, Right MCA TCD demonstrates normal flow velocities (arrow, C), which increased on day 4 (arrow, D). E and F, Repeat DSA 5 days after normal findings on the initial study demonstrates multifocal areas of constriction and dilation in the extracranial circulation (left external carotid artery injection, arrowheads, E) and intracranial circulation (vertebral injection, arrowheads, F).
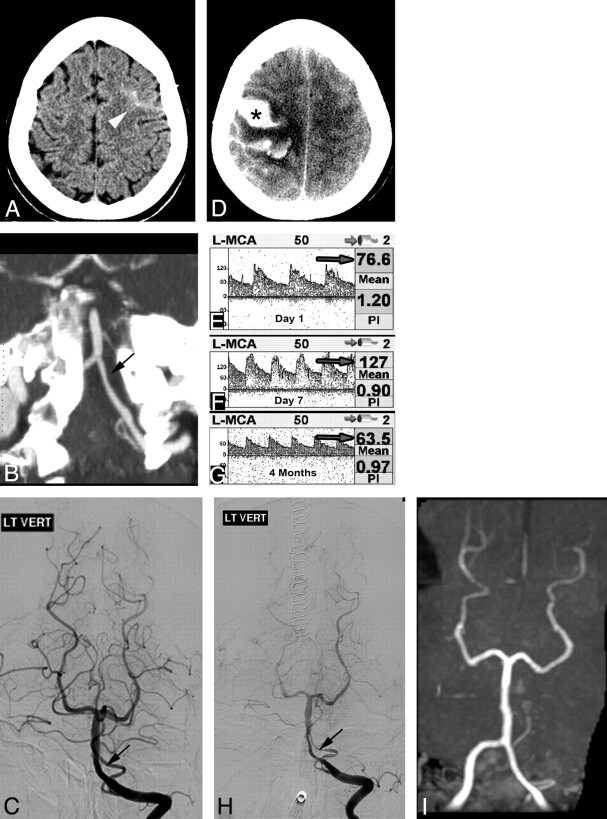
A, NCCT on admission shows convexal SAH (arrowhead). B and C, CTA, oblique coronal MIP reformat (B), suggests subtle left vertebral irregularity, but DSA findings are normal except for questionable irregularity in the left vertebral artery (arrow) not appreciated prospectively (C). E, TCD on admission demonstrates mildly elevated left MCA flow velocity (arrow). D, Repeat NCCT at day 5 demonstrates new IPH (asterisk) with worsened mass effect. F, TCD on day 7 demonstrates increased flow velocity consistent with vasospasm (arrow). H, Repeat DSA shows marked segmental vasoconstriction and poor contrast opacification of vessels. Follow-up TCD at 4 months (G) demonstrates normalization of flow velocities, and MRA shows resolution of vascular abnormalities (I).
References
-
- Call GK, Fleming MC, Sealfon S, et al. . Reversible cerebral segmental vasoconstriction. Stroke 1988;19:1159–70 - PubMed
-
- Ducros A, Boukobza M, Porcher R, et al. . The clinical and radiological spectrum of reversible cerebral vasoconstriction syndrome: a prospective series of 67 patients. Brain 2007;130:3091–101 - PubMed
-
- Calabrese LH, Dodick DW, Schwedt TJ, et al. . Narrative review: reversible cerebral vasoconstriction syndromes. Ann Intern Med 2007;146:34–44 - PubMed
-
- Gerretsen P, Kern RZ. Reversible cerebral vasoconstriction syndrome or primary angiitis of the central nervous system? Can J Neurol Sci 2007;34:467–77 - PubMed
-
- Chen SP, Fuh JL, Wang SJ, et al. . Magnetic resonance angiography in reversible cerebral vasoconstriction syndromes. Ann Neurol 2010;67:648–56 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical