

Implications of lowering threshold of plasma troponin concentration in diagnosis of myocardial infarction: cohort study
- PMID: 22422871
- PMCID: PMC3307810
- DOI: 10.1136/bmj.e1533
Implications of lowering threshold of plasma troponin concentration in diagnosis of myocardial infarction: cohort study
Abstract
Objective: To assess the relation between troponin concentration, assay precision, and clinical outcomes in patients with suspected acute coronary syndrome.
Design: Cohort study.
Setting: Tertiary centre in Scotland.
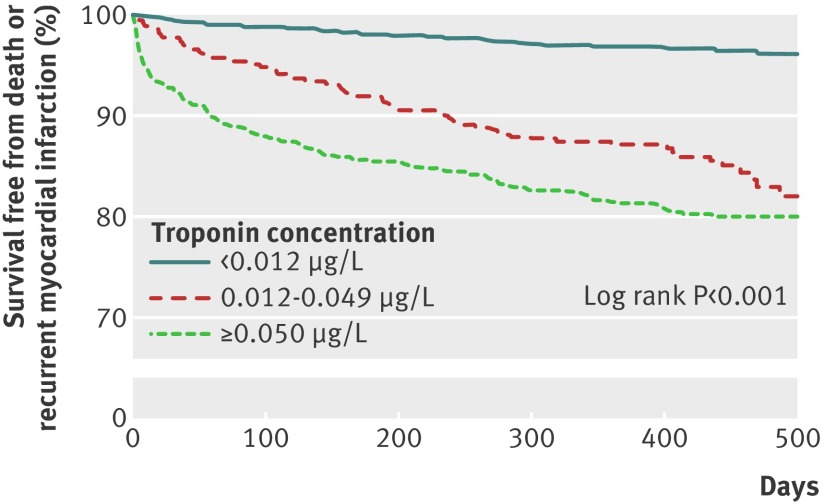
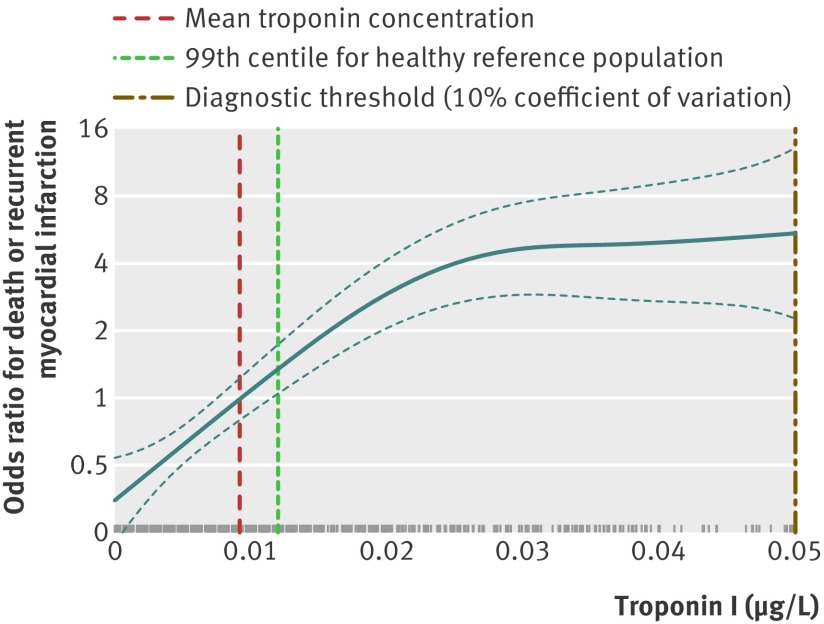
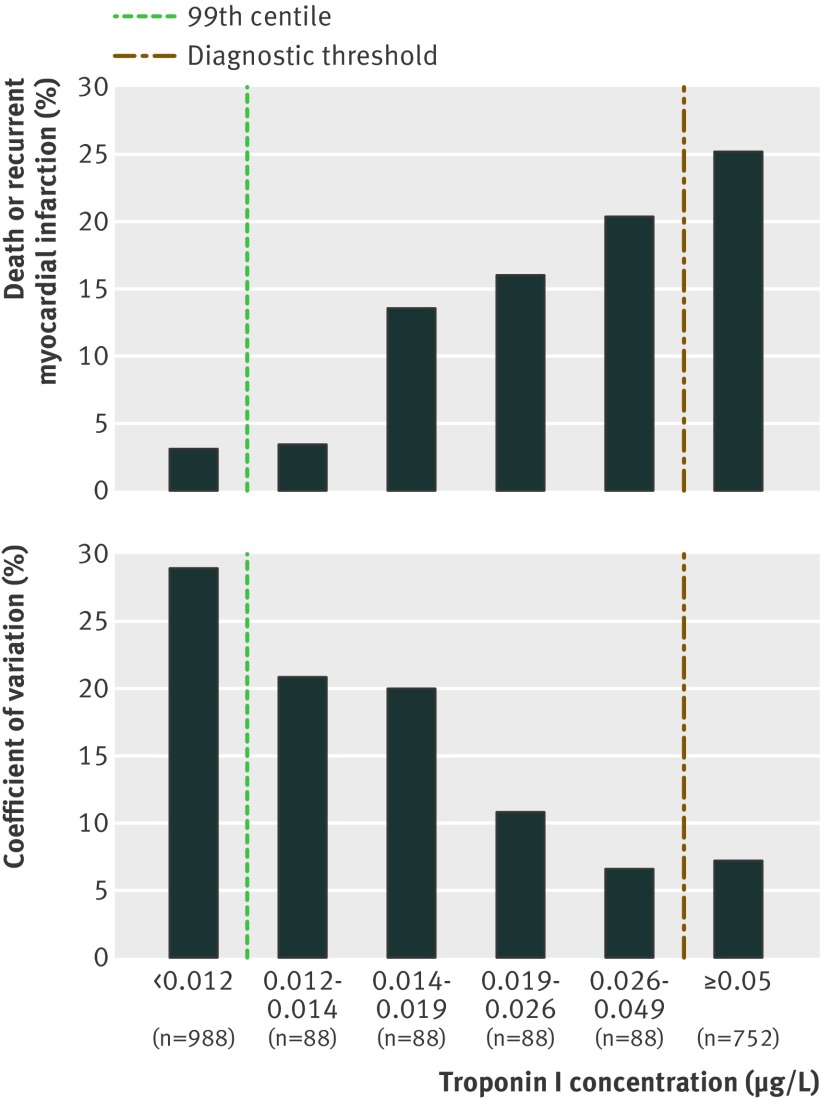
Participants: 2092 consecutive patients admitted with suspected acute coronary syndrome were stratified with a sensitive troponin I assay into three groups (<0.012, 0.012-0.049, and ≥0.050 µg/L) based on the 99th centile for troponin concentration (0.012 µg/L; coefficient of variation 20.8%) and the diagnostic threshold (0.050 µg/L; 7.2%).
Main outcome measure: One year survival without events (recurrent myocardial infarction, death) in patients grouped by troponin concentration.
Results: Troponin I concentrations were <0.012 µg/L in 988 patients (47%), 0.012-0.049 µg/L in 352 patients (17%), and ≥0.050 µg/L in 752 patients (36%). Adoption of the 99th centile would increase the number of people receiving a diagnosis of myocardial infarction from 752 to 1104: a relative increase of 47%. At one year, patients with troponin concentrations of 0.012-0.049 µg/L were more likely to be dead or readmitted with recurrent myocardial infarction than those with troponin concentrations <0.012 µg/L (13% v 3%, P<0.001; odds ratio 4.7, 95% confidence interval 2.9 to 7.9). Compared with troponin ≥0.050 µg/L, patients with troponin 0.012-0.049 µg/L had a higher risk profile but were less likely to have a diagnosis of, or be investigated and treated for, acute coronary syndrome.
Conclusion: Lowering the diagnostic threshold to the 99th centile and accepting greater assay imprecision would identify more patients with acute coronary syndrome at risk of recurrent myocardial infarction and death but would increase the diagnosis of myocardial infarction by 47%. It remains to be established whether reclassification of these patients and treatment for myocardial infarction would improve outcome.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
New guidance for troponin assays.BMJ. 2012 Mar 15;344:e1736. doi: 10.1136/bmj.e1736. BMJ. 2012. PMID: 22422833 No abstract available.
References
-
- Thygesen K, Alpert JS, White HD, Jaffe AS, Apple FS, Galvani M, et al. Universal definition of myocardial infarction. Circulation 2007;116:2634-53. - PubMed
-
- Bauer A, Gawaz M. Sensitive cardiac troponin assays. N Engl J Med 2009;361:2575-7. - PubMed
-
- Morrow DA, Cannon CP, Jesse RL, Newby LK, Ravkilde J, Storrow AB, et al. National Academy of Clinical Biochemistry Laboratory Medicine Practice Guidelines: clinical characteristics and utilization of biochemical markers in acute coronary syndromes. Clin Chem 2007;53:552-74. - PubMed
-
- Mills NL, Churchhouse AM, Lee KK, Anand A, Gamble D, Shah AS, et al. Implementation of a sensitive troponin I assay and risk of recurrent myocardial infarction and death in patients with suspected acute coronary syndrome. JAMA 2011;305:1210-6. - PubMed
-
- Jaffe AS, Apple FS, Morrow DA, Lindahl B, Katus HA. Being rational about (im)precision: a statement from the Biochemistry Subcommittee of the Joint European Society of Cardiology/American College of Cardiology Foundation/American Heart Association/World Heart Federation Task Force for the definition of myocardial infarction. Clin Chem 2010;56:941-3. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical