

doi: 10.4329/wjr.v4.i2.53.
Primary lymphoma of the liver - A complex diagnosis
Affiliations
- PMID: 22423319
- PMCID: PMC3304094
- DOI: 10.4329/wjr.v4.i2.53
Item in Clipboard
Primary lymphoma of the liver - A complex diagnosis
World J Radiol.
.
Abstract
A 59-year-old woman presented with the clinical symptoms and radiologic investigations of a liver lesion suspect of metastasis. However, postoperative histopathology revealed a primary hepatic lymphoma (PHL). The case of a patient with a solitary PHL, which was treated by resection and subsequent chemotherapy, will be discussed with a short overview of the literature.
Keywords: Computed tomography; Diagnosis; Hepatic; Liver; Lymphoma; Magnetic resonance imaging; Primary.
Figures
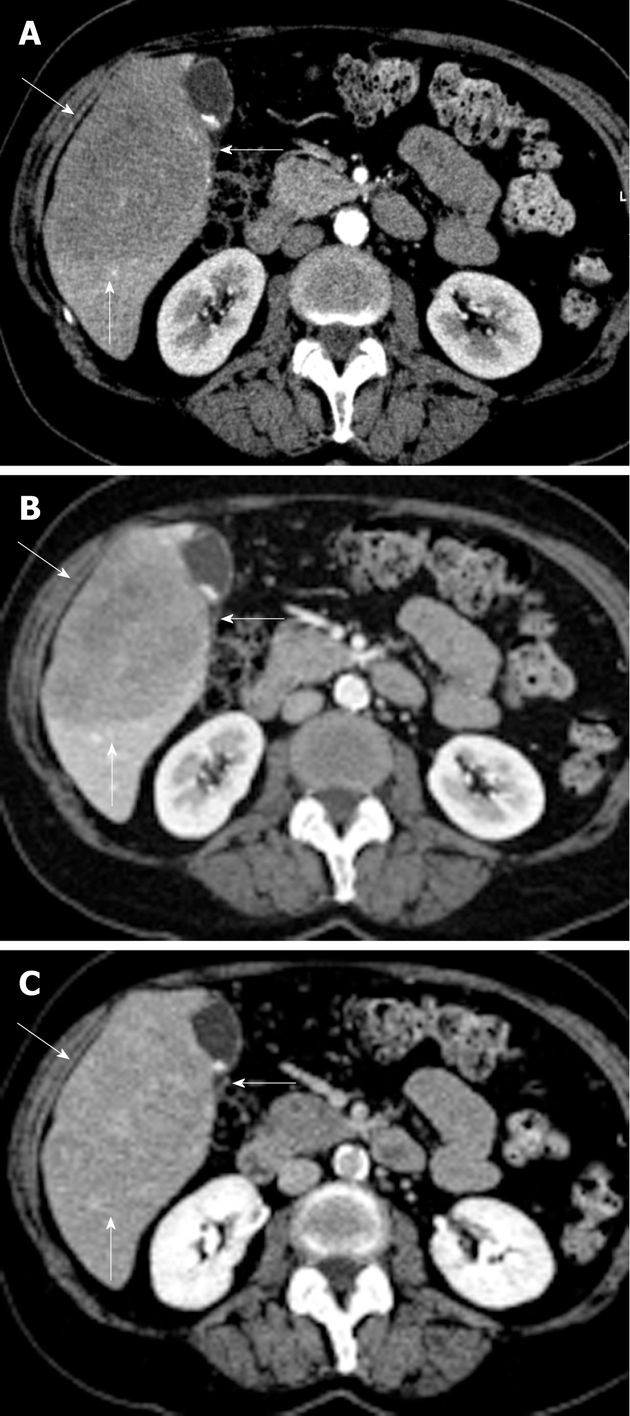
Radiological depiction of the liver lesion. Arterial (A), portal (B) and equilibrium phase (C) computed tomography scan with a large (10 cm × 8 cm × 7.5 cm) hypovascular lesion in segments V and VI of the liver with some inhomogeneity and without calcifications (lesion indicated by 3 white arrows).
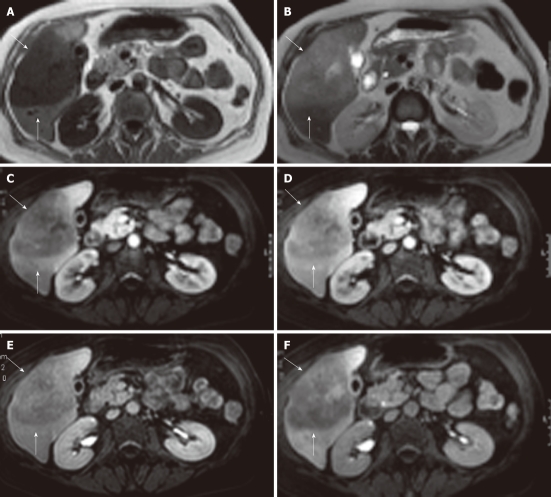
Magnetic resonance imaging showing a large, sharply demarcated lesion measuring 11 cm in the right liver lobe. The lesion is hypointense on T1 (A) and hyperintense on T2 (B) weighed images with slight inhomogeneity. Arterial (C), portal (D), equilibrium (E) and hepato-biliary (20 min) (F) phase magnetic resonance imaging after Gd-EOB-DTPA contrast enhancement reveal a hypovasular lesion without uptake in the hepato-biliary phase (lesion indicated by white arrows).
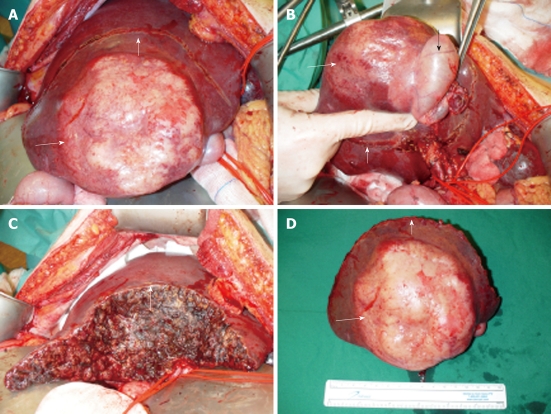
Intraoperative aspect of lesion. A: Tumor presentation intra-operatively; B: Tumor in segment V/VI of the liver with en bloc in the resection specimen the gall bladder (black arrow indicates gall bladder); C: Resection plane of the liver; D: Resection specimen with centrally white/yellow shiny tumor (small white arrow indicates resection plane, long white arrow indicates tumor).
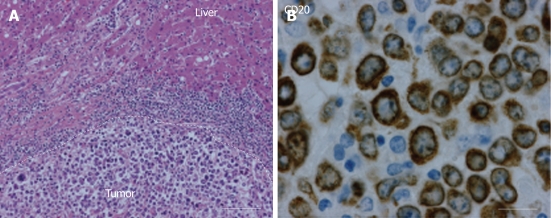
Histopathological results. A: Hematoxylin eosin staining (150 ×) shows a large cell malignancy with mostly loose tumor cells with nuclear polymorphism. Furthermore, frequent giant nuclear bodies with macro-nucleoli and numerous cell mitoses. No central necrosis is observed; B: A photomicrograph (400 ×) showing lymphocytic tumor cells which are positive for CD20 staining around the plasma membrane, indicating non-Hodgkin lymphoma of B-cell origin.
References
-
- Sehn LH, Donaldson J, Chhanabhai M, Fitzgerald C, Gill K, Klasa R, MacPherson N, O’Reilly S, Spinelli JJ, Sutherland J, et al. Introduction of combined CHOP plus rituximab therapy dramatically improved outcome of diffuse large B-cell lymphoma in British Columbia. J Clin Oncol. 2005;23:5027–5033. - PubMed
-
- Ata AA, Kamel IA. Primary reticulum cell sarcoma of the liver. A case report. J Egypt Med Assoc. 1965;48:514–521. - PubMed
-
- Caccamo D, Pervez NK, Marchevsky A. Primary lymphoma of the liver in the acquired immunodeficiency syndrome. Arch Pathol Lab Med. 1986;110:553–555. - PubMed
-
- Freeman C, Berg JW, Cutler SJ. Occurrence and prognosis of extranodal lymphomas. Cancer. 1972;29:252–260. - PubMed
-
- Craig JR, Peters RL, Edmondson HA. Tumors of the liver and intrahepatic bile ducts. 2nd Series. Washington, DC: Armed Forces Institute of Pathology; 1989. pp. 244–246.
LinkOut - more resources
Full Text Sources
