

Study design for the Immediate Myocardial Metabolic Enhancement During Initial Assessment and Treatment in Emergency Care (IMMEDIATE) Trial: A double-blind randomized controlled trial of intravenous glucose, insulin, and potassium for acute coronary syndromes in emergency medical services
- PMID: 22424000
- PMCID: PMC4009621
- DOI: 10.1016/j.ahj.2012.02.002
Study design for the Immediate Myocardial Metabolic Enhancement During Initial Assessment and Treatment in Emergency Care (IMMEDIATE) Trial: A double-blind randomized controlled trial of intravenous glucose, insulin, and potassium for acute coronary syndromes in emergency medical services
Abstract
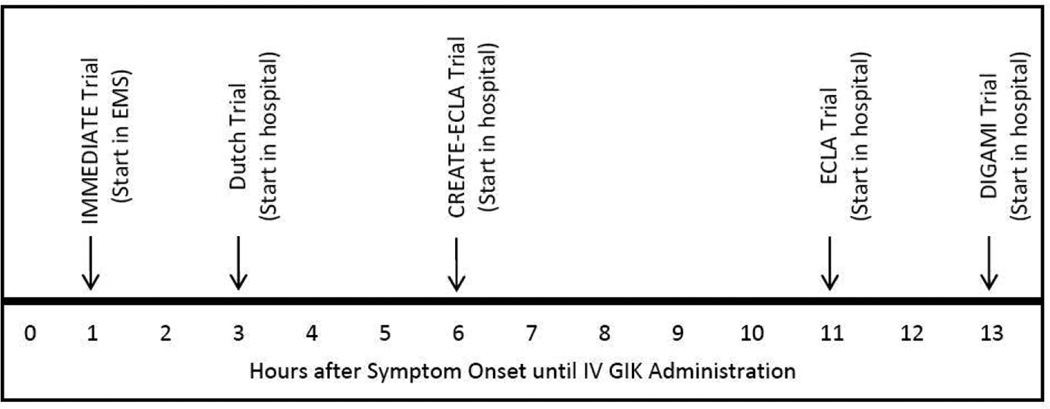
Background: Experimental studies suggest that metabolic myocardial support by intravenous (IV) glucose, insulin, and potassium (GIK) reduces ischemia-induced arrhythmias, cardiac arrest, mortality, progression from unstable angina pectoris to acute myocardial infarction (AMI), and myocardial infarction size. However, trials of hospital administration of IV GIK to patients with ST-elevation myocardial infarction (STEMI) have generally not shown favorable effects possibly because of the GIK intervention taking place many hours after ischemic symptom onset. A trial of GIK used in the very first hours of ischemia has been needed, consistent with the timing of benefit seen in experimental studies.
Objective: The IMMEDIATE Trial tested whether, if given very early, GIK could have the impact seen in experimental studies. Accordingly, distinct from prior trials, IMMEDIATE tested the impact of GIK (1) in patients with acute coronary syndromes (ACS), rather than only AMI or STEMI, and (2) administered in prehospital emergency medical service settings, rather than later, in hospitals, after emergency department evaluation.
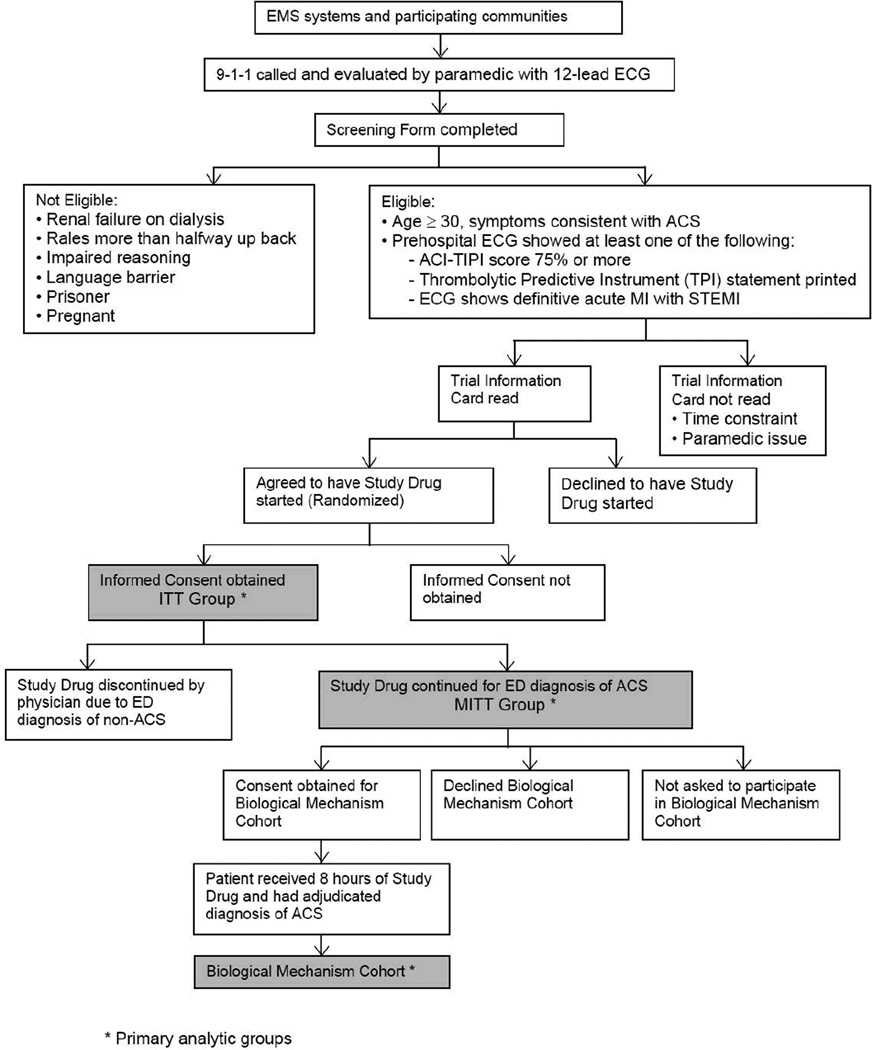
Design: The IMMEDIATE Trial was an emergency medical service-based randomized placebo-controlled clinical effectiveness trial conducted in 13 cities across the United States that enrolled 911 participants. Eligible were patients 30 years or older for whom a paramedic performed a 12-lead electrocardiogram to evaluate chest pain or other symptoms suggestive of ACS for whom electrocardiograph-based acute cardiac ischemia time-insensitive predictive instrument indicated a ≥75% probability of ACS, and/or the thrombolytic predictive instrument indicated the presence of a STEMI, or if local criteria for STEMI notification of receiving hospitals were met. Prehospital IV GIK or placebo was started immediately. Prespecified were the primary end point of progression of ACS to infarction and, as major secondary end points, the composite of cardiac arrest or in-hospital mortality, 30-day mortality, and the composite of cardiac arrest, 30-day mortality, or hospitalization for heart failure. Analyses were planned on an intent-to-treat basis, on a modified intent-to-treat group who were confirmed in emergency departments to have ACS, and for participants presenting with STEMI.
Conclusion: The IMMEDIATE Trial tested whether GIK, when administered as early as possible in the course of ACS by paramedics using acute cardiac ischemia time-insensitive predictive instrument and thrombolytic predictive instrument decision support, would reduce progression to AMI, mortality, cardiac arrest, and heart failure. It also tested whether it would provide clinical and pathophysiologic information on GIK's biological mechanisms.
Copyright © 2012 Mosby, Inc. All rights reserved.
Figures
References
-
- Oliver MF, Opie LH. Effects of glucose and fatty acids on myocardial ischemia and arrhythmias. Lancet. 1994;343:155–158. - PubMed
-
- Oliver MF. Sudden unexpected cardiac death. Eur Heart J. 2002;23:1797–1798. - PubMed
-
- Fath-Ordoubadi F, Beatt KJ. Glucose-Insulin-Potassium (GIK) therapy for treatment of acute myocardial infarction: An overview of randomized placebo controlled trials. Circulation. 1997;96:1152–1156. - PubMed
-
- Rackley CE, Russell RO, Rogers WJ, Mantle JA, McDaniel HG, Papapietro SE. Clinical experience with glucose-insulin-potassium therapy in acute myocardial infarction. Am Heart J. 1981;102:1038–1049. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
