

Changes in initial expenditures for benign prostatic hyperplasia evaluation in the Medicare population: a comparison to overall Medicare inflation
- PMID: 22425128
- PMCID: PMC3539409
- DOI: 10.1016/j.juro.2011.12.079
Changes in initial expenditures for benign prostatic hyperplasia evaluation in the Medicare population: a comparison to overall Medicare inflation
Abstract
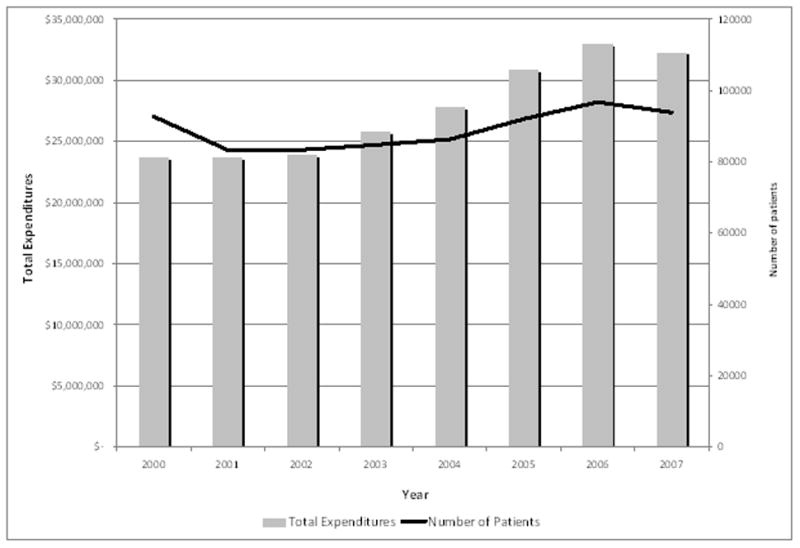
Purpose: Benign prostatic hyperplasia creates significant expenses for the Medicare program. We determined expenditure trends for benign prostatic hyperplasia evaluative testing after urologist consultation and placed these trends in the context of overall Medicare expenditures.
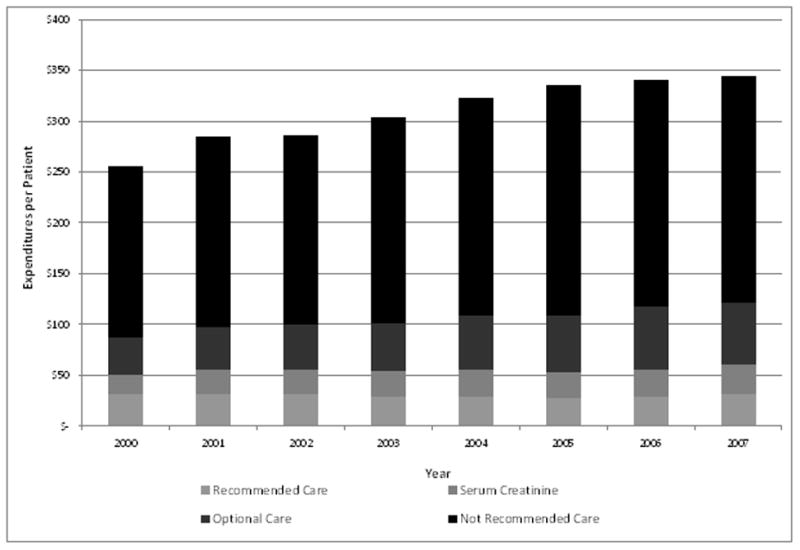
Materials and methods: Using a 5% national sample of Medicare beneficiaries from 2000 to 2007 we developed a cohort of 40,253 with claims for new visits to urologists for diagnoses consistent with symptomatic benign prostatic hyperplasia. We assessed trends in initial inflation and geography adjusted expenditures within 12 months of diagnosis by evaluative test categories derived from the 2003 American Urological Association guideline on the management of benign prostatic hyperplasia. Using governmental reports on Medicare expenditure trends for benign prostatic hyperplasia we compared expenditures to overall and imaging specific Medicare expenditures. Comparisons were assessed by the Z-test and regression analysis for linear trends, as appropriate.
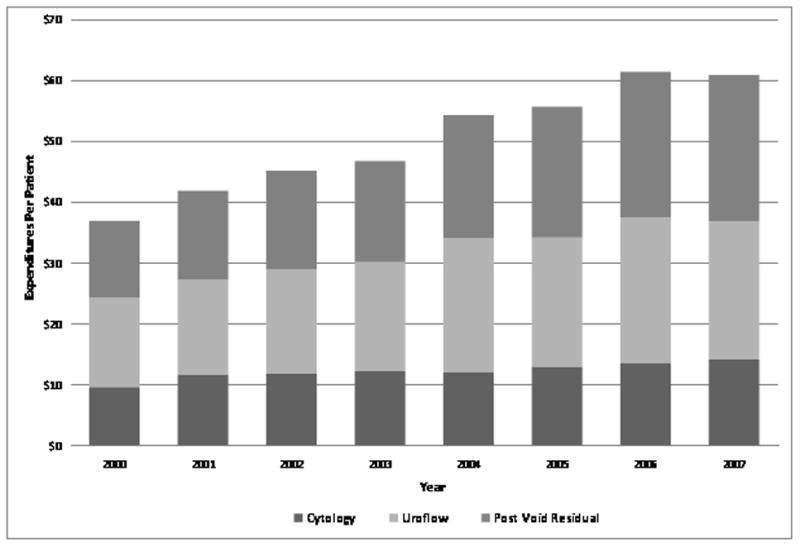
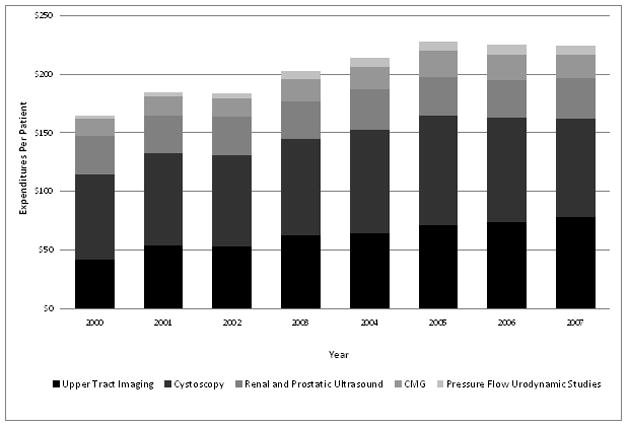
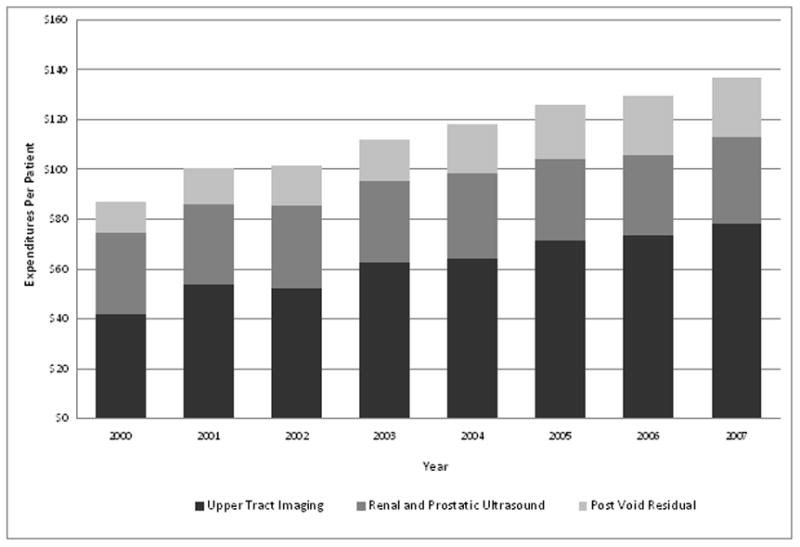
Results: Between 2000 and 2007 inflation adjusted total Medicare expenditures per patient for the initial evaluation of patients with benign prostatic hyperplasia seen by urologists increased from $255.44 to $343.98 (p <0.0001). Benign prostatic hyperplasia related imaging increases were significantly less than overall Medicare imaging expenditure increases (55% vs 104%, p <0.001). The increase in per patient expenditures for benign prostatic hyperplasia was significantly lower than the increase in overall Medicare expenditures per enrollee (35% vs 45%, p = 0.0015).
Conclusions: From 2000 to 2007 inflation adjusted expenditures increased for benign prostatic hyperplasia related evaluations. This growth was slower than the overall growth in Medicare expenditures. The increase in BPH related imaging expenditures was restrained compared to that of the Medicare program as a whole.
Copyright © 2012 American Urological Association Education and Research, Inc. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Roehrborn C, McConnell J, Barry M. American Urological Association Guideline on the Management of Benign Prostatic Hyperplasia (BPH) American Urological Association; 2003.
-
- Wei JT, Calhoun E, Jacobsen SJ. Urologic diseases in America project: benign prostatic hyperplasia. J Urol. 2005;173:1256. - PubMed
-
- Warren JL, Klabunde CN, Schrag D, et al. Overview of the SEER-Medicare data: content, research applications, and generalizability to the United States elderly population. Med Care. 2002;40:IV. - PubMed
-
- Geithner T, Solis H, Sebelius K, et al. D. o. H. a. H. Services, editor. ANNUAL REPORT OF THE BOARDS OF TRUSTEES OF THE FEDERAL HOSPITAL INSURANCE AND FEDERAL SUPPLEMENTARY MEDICAL INSURANCE TRUST FUNDS. Washington, DC: 2011.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
