

Feasibility, safety, acceptability, and yield of office-based, screening transnasal esophagoscopy (with video)
- PMID: 22425272
- PMCID: PMC4154478
- DOI: 10.1016/j.gie.2012.01.021
Feasibility, safety, acceptability, and yield of office-based, screening transnasal esophagoscopy (with video)
Abstract
Background: Endoscopic screening for esophageal neoplasia can identify patients eligible for early intervention for precancerous lesions. Unsedated transnasal esophagoscopy may provide an efficient and accurate endoscopic assessment with fewer risks and less cost, compared with conventional upper endoscopy.
Objective: To assess the feasibility, safety, acceptability, and yield of unsedated transnasal esophagoscopy in a primary care population.
Design: Multicenter, prospective, cross-sectional study.
Setting: Two outpatient tertiary-care centers.
Patients: This study involved a general medical clinic population aged between 40 and 85 years.
Intervention: Unsedated, office-based transnasal esophagoscopy.
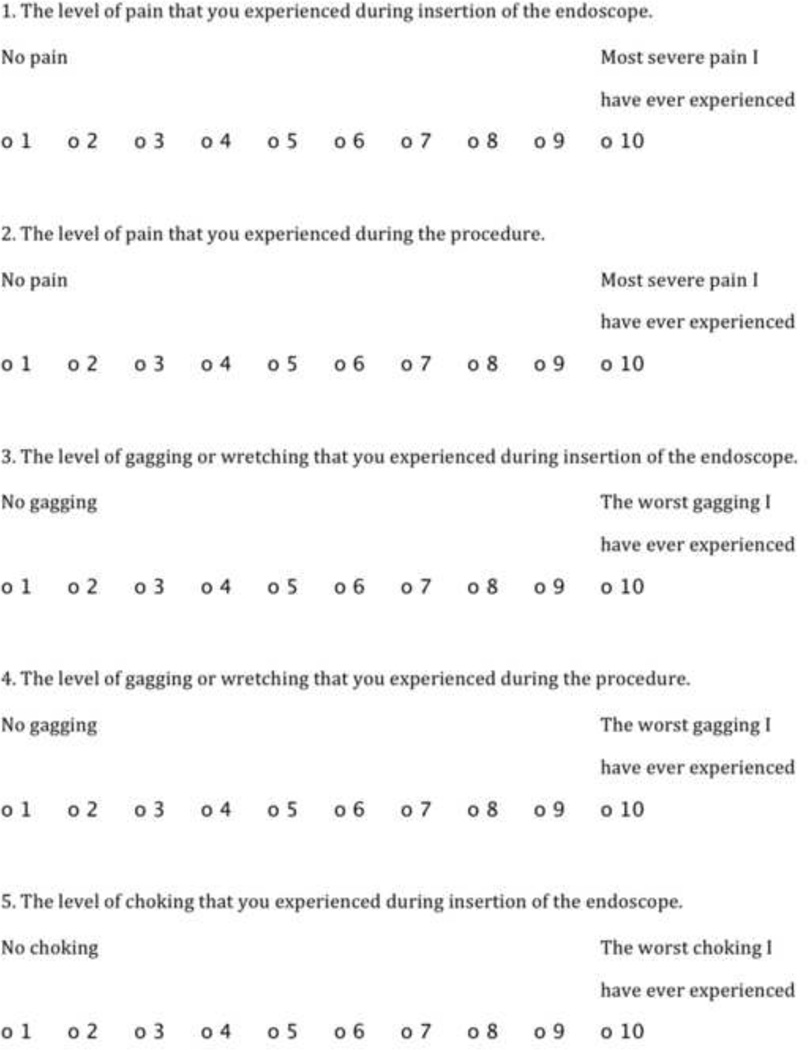
Main outcome measurements: Procedure yield; completeness of examination; procedure length; adverse events and complications; choking, gagging, pain, or anxiety during the examination; and overall tolerability.
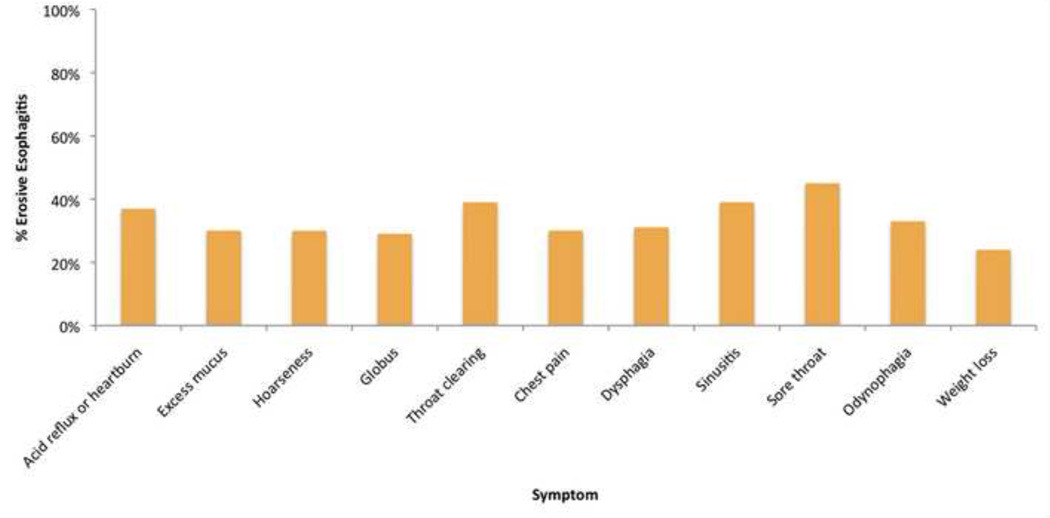
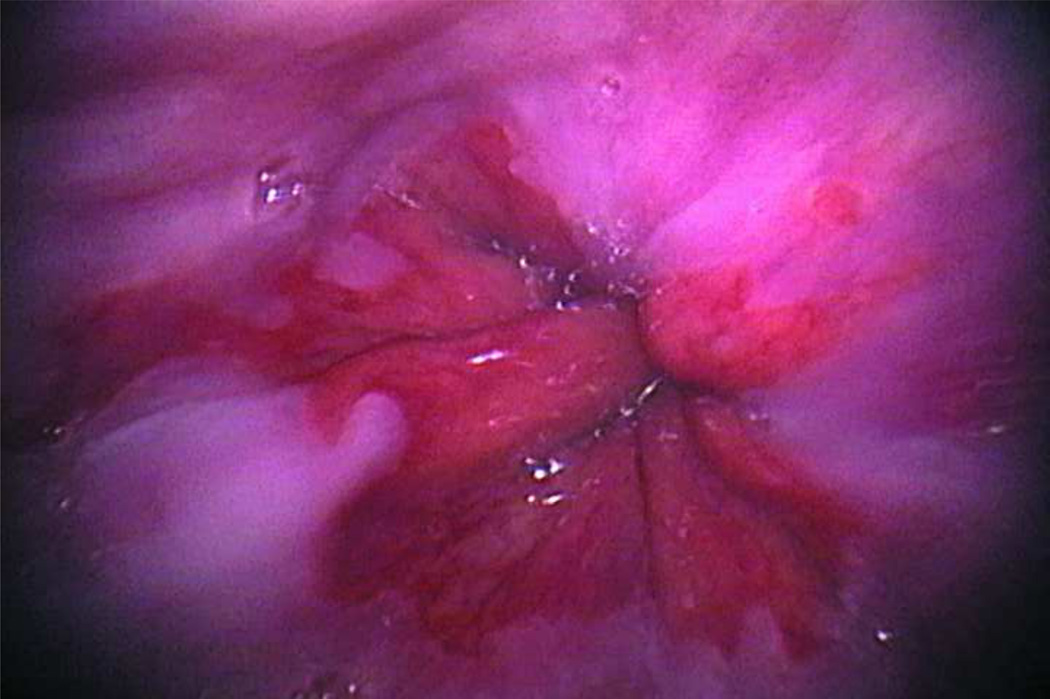
Results: A total of 426 participants (mean [± standard deviation] age 55.8 ± 9.5 years; 43% male) enrolled in the study, and 422 (99%) completed the examination. Mean (± standard deviation) examination time was 3.7 ± 1.8 minutes. There were no serious adverse events, and 12 participants (2.8%) reported minor complications. Participants reported minimal choking, gagging, pain, or anxiety. The examination was well-tolerated by most participants. Overall, 38% of participants had an esophageal finding that changed management (34% erosive esophagitis, 4% Barrett's esophagus).
Limitations: Nonrandomized study, tertiary-care centers only, self-selected population with a large proportion reporting esophageal symptoms.
Conclusion: Unsedated transnasal esophagoscopy is a feasible, safe, and well-tolerated method to screen for esophageal disease in a primary care population. Endoscopic findings are common in this patient population.
Copyright © 2012 American Society for Gastrointestinal Endoscopy. Published by Mosby, Inc. All rights reserved.
Figures
Comment in
-
Ultrathin transnasal endoscopy without sedation: the straight skinny.Gastrointest Endosc. 2012 May;75(5):962-4. doi: 10.1016/j.gie.2012.02.032. Gastrointest Endosc. 2012. PMID: 22520876 No abstract available.
References
-
- Pohl H, Welch HG. The role of overdiagnosis and reclassification in the marked increase of esophageal adenocarcinoma incidence. J Natl Cancer Inst. 2005;97:142–146. - PubMed
-
- Pohl H, Sirovich B, Welch HG. Esophageal adenocarcinoma incidence: are we reaching the peak? Cancer Epidemiol Biomarkers Prev. 2010;19:1468–1470. - PubMed
-
- Sharma VK, Nguyen CC, Crowell MD, Lieberman DA, de Garmo P, Fleischer DE. A national study of cardiopulmonary unplanned events after GI endoscopy. Gastrointest Endosc. 2007;66:27–34. - PubMed
-
- Dulai GS, Guha S, Kahn KL, Gornbein J, Weinstein WM. Preoperative prevalence of Barrett's esophagus in esophageal adenocarcinoma: a systematic review. Gastroenterology. 2002;122:26–33. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
