

Determinants of adverse events in vascular surgery
- PMID: 22425449
- PMCID: PMC4890555
- DOI: 10.1016/j.jamcollsurg.2012.01.045
Determinants of adverse events in vascular surgery
Abstract
Background: Patient safety is a national priority. Patient Safety Indicators (PSIs) monitor potential adverse events during hospital stays. Surgical specialty PSI benchmarks do not exist, and are needed to account for differences in the range of procedures performed, reasons for the procedure, and differences in patient characteristics. A comprehensive profile of adverse events in vascular surgery was created.
Study design: The Nationwide Inpatient Sample was queried for 8 vascular procedures using ICD-9-CM codes from 2005 to 2009. Factors associated with PSI development were evaluated in univariate and multivariate analyses.
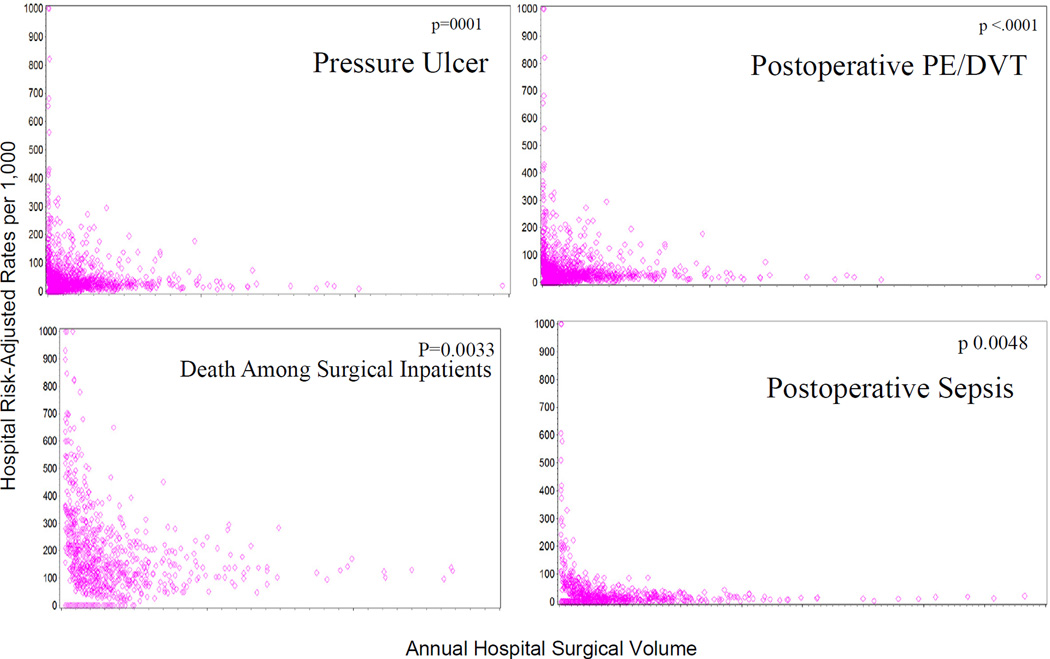
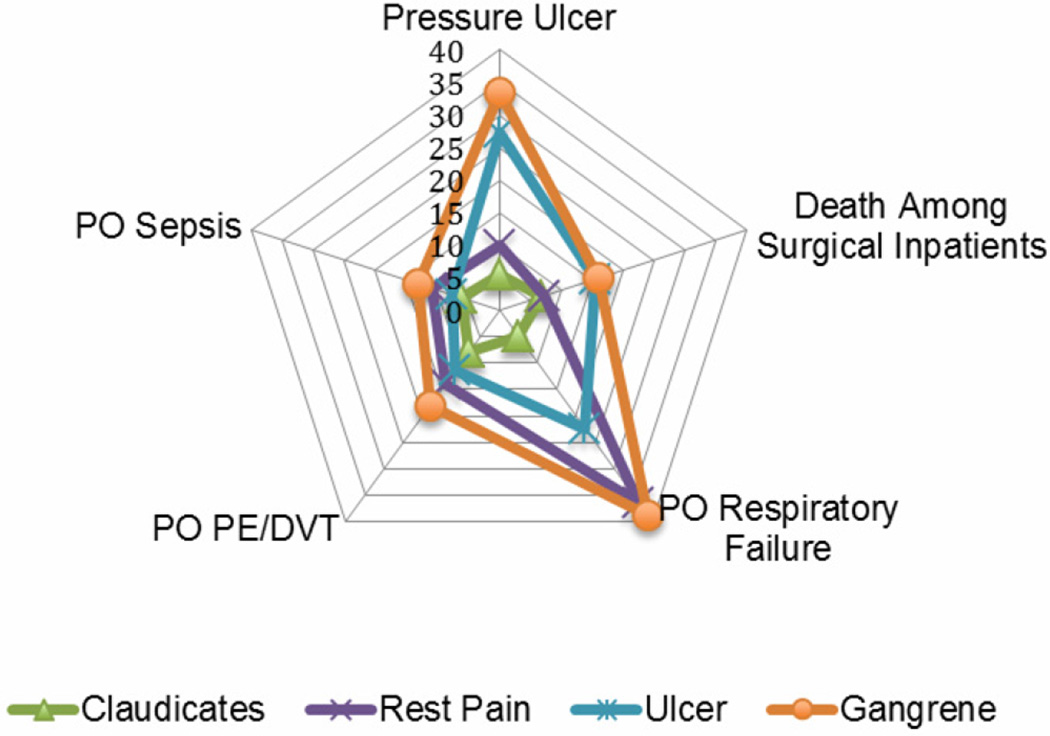
Results: A total of 1,412,703 patients underwent a vascular procedure and a PSI developed in 5.2%. PSIs were more frequent in female, nonwhite patients with public payers (p < 0.01). Patients at mid and low-volume hospitals had greater odds of developing a PSI (odds ratio [OR] = 1.17; 95% CI, 1.10-1.23 and OR = 1.69; 95% CI, 1.53-1.87). Amputations had highest PSI risk-adjusted rate and carotid endarterectomy and endovascular abdominal aortic aneurysm repair had lower risk-adjusted rate (p < 0.0001). PSI risk-adjusted rate increased linearly by severity of patient indication: claudicants (OR = 0.40; 95% CI, 0.35-0.46), rest pain patients (OR = 0.78; 95% CI, 0.69-0.90), ulcer (OR = 1.20; 95% CI, 1.07-1.34), and gangrene patients (OR = 1.85; 95% CI, 1.66-2.06).
Conclusions: Patient safety events in vascular surgery were high and varied by procedure, with amputations and open abdominal aortic aneurysm repair having considerably more potential adverse events. PSIs were associated with black race, public payer, and procedure indication. It is important to note the overall higher rates of PSIs occurring in vascular patients and to adjust benchmarks for this surgical specialty appropriately.
Copyright © 2012 American College of Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Kohn KT, Corrigan JM, Donaldson MS. To Err is Human: Building a Safer Health System. Washington DC: Institutes of Medicine, National Academy Press; 1999. - PubMed
-
- Zhan C, Miller MR. Excess length of stay, charges, and mortality attributable to medical injuries during hospitalization. JAMA. 2003;290:1868–1874. - PubMed
-
- Rivard PE, Luther SL, Christiansen CL, et al. Using patient safety indicators to estimate the impact of potential adverse events on outcomes. Med Care Res Rev. 2008;65:67–87. - PubMed
-
- Friedman B, Encinosa W, Jiang HJ, Mutter R. Do patient safety events increase readmissions? Med Care. 2009;47:583–590. - PubMed
-
- Vogel TR, Dombrovskiy VY, Haser PB, Graham AM. Evaluating preventable adverse safety events after elective lower extremity procedures. J Vasc Surg. 2011 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
